
2025 Dental Summary
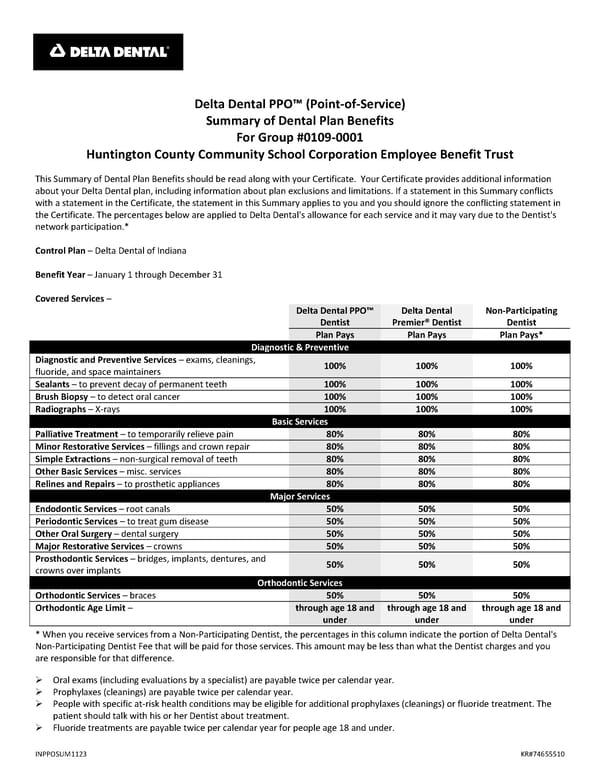
Delta Dental PPO™ (Point‐of‐Service) Summary of Dental Plan Benefits For Group #0109‐0001 Huntington County Community School Corporation Employee Benefit Trust This Summary of Dental Plan Benefits should be read along with your Certificate. Your Certificate provides additional information about your Delta Dental plan, including information about plan exclusions and limitations. If a statement in this Summary conflicts with a statement in the Certificate, the statement in this Summary applies to you and you should ignore the conflicting statement in the Certificate. The percentages below are applied to Delta Dental's allowance for each service and it may vary due to the Dentist's network participation.* Control Plan – Delta Dental of Indiana Benefit Year – January 1 through December 31 Covered Services – Delta Dental PPO™ Delta Dental Non‐Participating Dentist Premier® Dentist Dentist Plan Pays Plan Pays Plan Pays* Diagnostic & Preventive Diagnostic and Preventive Services – exams, cleanings, 100% 100% 100% fluoride, and space maintainers Sealants – to prevent decay of permanent teeth 100% 100% 100% Brush Biopsy – to detect oral cancer 100% 100% 100% Radiographs – X‐rays 100% 100% 100% Basic Services Palliative Treatment – to temporarily relieve pain 80% 80% 80% Minor Restorative Services – fillings and crown repair 80% 80% 80% Simple Extractions – non‐surgical removal of teeth 80% 80% 80% Other Basic Services – misc. services 80% 80% 80% Relines and Repairs – to prosthetic appliances 80% 80% 80% Major Services Endodontic Services – root canals 50% 50% 50% Periodontic Services – to treat gum disease 50% 50% 50% Other Oral Surgery – dental surgery 50% 50% 50% Major Restorative Services – crowns 50% 50% 50% Prosthodontic Services – bridges, implants, dentures, and 50% 50% 50% crowns over implants Orthodontic Services Orthodontic Services – braces 50% 50% 50% Orthodontic Age Limit – through age 18 and through age 18 and through age 18 and under under under * When you receive services from a Non‐Participating Dentist, the percentages in this column indicate the portion of Delta Dental's Non‐Participating Dentist Fee that will be paid for those services. This amount may be less than what the Dentist charges and you are responsible for that difference. exams (including evaluations by a specialist) are payable twice per calendar year. Oral Prophylaxes (cleanings) are payable twice per calendar year. People with specific at‐risk health conditions may be eligible for additional prophylaxes (cleanings) or fluoride treatment. The patient should talk with his or her Dentist about treatment. Fluoride treatments are payable twice per calendar year for people age 18 and under. INPPOSUM1123 KR#74655510
 2025 Dental Summary Page 2
2025 Dental Summary Page 2