
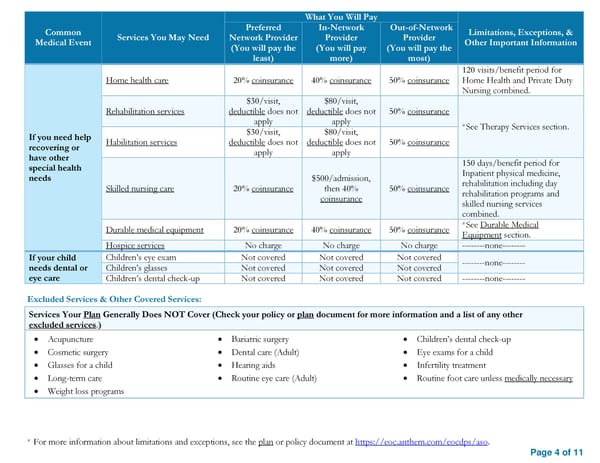
What You Will Pay Common Preferred In-Network Out-of-Network Limitations, Exceptions, & Medical Event Services You May Need Network Provider Provider Provider Other Important Information (You will pay the (You will pay (You will pay the least) more) most) 120 visits/benefit period for Home health care 20% coinsurance 40% coinsurance 50% coinsurance Home Health and Private Duty Nursing combined. $30/visit, $80/visit, Rehabilitation services deductible does not deductible does not 50% coinsurance apply apply *See Therapy Services section. If you need help $30/visit, $80/visit, recovering or Habilitation services deductible does not deductible does not 50% coinsurance have other apply apply special health 150 days/benefit period for needs $500/admission, Inpatient physical medicine, Skilled nursing care 20% coinsurance then 40% 50% coinsurance rehabilitation including day coinsurance rehabilitation programs and skilled nursing services combined. Durable medical equipment 20% coinsurance 40% coinsurance 50% coinsurance *See Durable Medical Equipment section. Hospice services No charge No charge No charge --------none-------- If your child Children’s eye exam Not covered Not covered Not covered --------none-------- needs dental or Children’s glasses Not covered Not covered Not covered eye care Children’s dental check-up Not covered Not covered Not covered --------none-------- Excluded Services & Other Covered Services: Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.) • Acupuncture • Bariatric surgery • Children’s dental check-up • Cosmetic surgery • Dental care (Adult) • Eye exams for a child • Glasses for a child • Hearing aids • Infertility treatment • Long-term care • Routine eye care (Adult) • Routine foot care unless medically necessary • Weight loss programs * For more information about limitations and exceptions, see the plan or policy document at https://eoc.anthem.com/eocdps/aso. Page 4 of 11
 2025 SBC HCCSC Anthem HealthSync PPO 2 Page 3 Page 5
2025 SBC HCCSC Anthem HealthSync PPO 2 Page 3 Page 5