
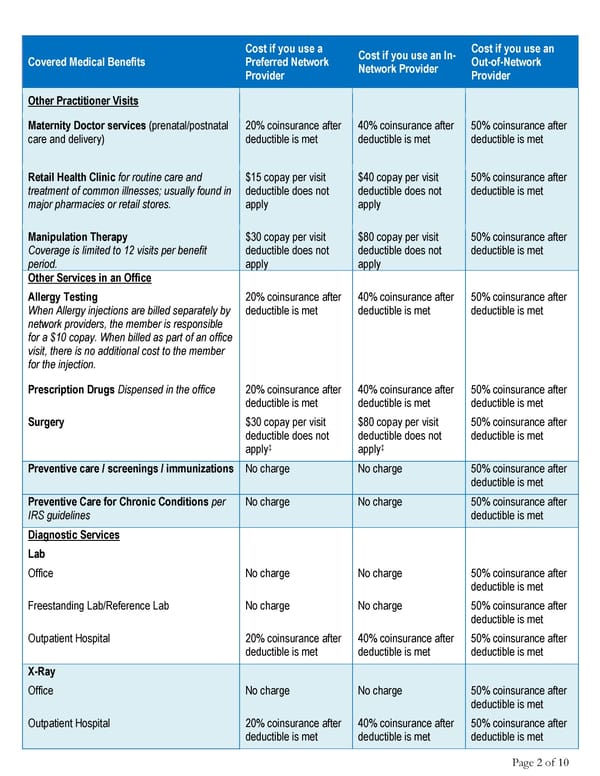
Cost if you use a Cost if you use an In- Cost if you use an Covered Medical Benefits Preferred Network Network Provider Out-of-Network Provider Provider Other Practitioner Visits Maternity Doctor services (prenatal/postnatal 20% coinsurance after 40% coinsurance after 50% coinsurance after care and delivery) deductible is met deductible is met deductible is met Retail Health Clinic for routine care and $15 copay per visit $40 copay per visit 50% coinsurance after treatment of common illnesses; usually found in deductible does not deductible does not deductible is met major pharmacies or retail stores. apply apply Manipulation Therapy $30 copay per visit $80 copay per visit 50% coinsurance after Coverage is limited to 12 visits per benefit deductible does not deductible does not deductible is met period. apply apply Other Services in an Office Allergy Testing 20% coinsurance after 40% coinsurance after 50% coinsurance after When Allergy injections are billed separately by deductible is met deductible is met deductible is met network providers, the member is responsible for a $10 copay. When billed as part of an office visit, there is no additional cost to the member for the injection. Prescription Drugs Dispensed in the office 20% coinsurance after 40% coinsurance after 50% coinsurance after deductible is met deductible is met deductible is met Surgery $30 copay per visit $80 copay per visit 50% coinsurance after deductible does not deductible does not deductible is met apply‡ apply‡ Preventive care / screenings / immunizations No charge No charge 50% coinsurance after deductible is met Preventive Care for Chronic Conditions per No charge No charge 50% coinsurance after IRS guidelines deductible is met Diagnostic Services Lab Office No charge No charge 50% coinsurance after deductible is met Freestanding Lab/Reference Lab No charge No charge 50% coinsurance after deductible is met Outpatient Hospital 20% coinsurance after 40% coinsurance after 50% coinsurance after deductible is met deductible is met deductible is met X-Ray Office No charge No charge 50% coinsurance after deductible is met Outpatient Hospital 20% coinsurance after 40% coinsurance after 50% coinsurance after deductible is met deductible is met deductible is met Page 2 of 10
 2025 Summary HCCSC Anthem HealthSync PPO 1 Page 1 Page 3
2025 Summary HCCSC Anthem HealthSync PPO 1 Page 1 Page 3