
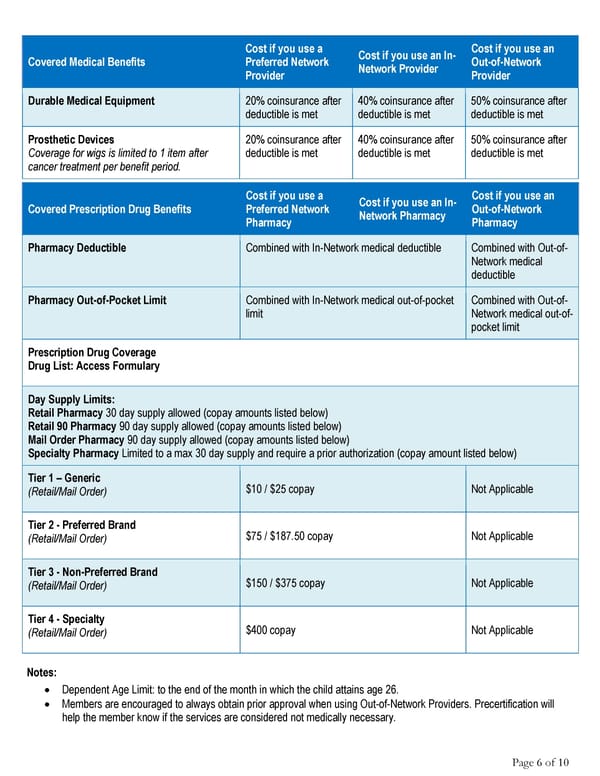
Cost if you use a Cost if you use an In- Cost if you use an Covered Medical Benefits Preferred Network Network Provider Out-of-Network Provider Provider Durable Medical Equipment 20% coinsurance after 40% coinsurance after 50% coinsurance after deductible is met deductible is met deductible is met Prosthetic Devices 20% coinsurance after 40% coinsurance after 50% coinsurance after Coverage for wigs is limited to 1 item after deductible is met deductible is met deductible is met cancer treatment per benefit period. Cost if you use a Cost if you use an In- Cost if you use an Covered Prescription Drug Benefits Preferred Network Network Pharmacy Out-of-Network Pharmacy Pharmacy Pharmacy Deductible Combined with In-Network medical deductible Combined with Out-of- Network medical deductible Pharmacy Out-of-Pocket Limit Combined with In-Network medical out-of-pocket Combined with Out-of- limit Network medical out-of- pocket limit Prescription Drug Coverage Drug List: Access Formulary Day Supply Limits: Retail Pharmacy 30 day supply allowed (copay amounts listed below) Retail 90 Pharmacy 90 day supply allowed (copay amounts listed below) Mail Order Pharmacy 90 day supply allowed (copay amounts listed below) Specialty Pharmacy Limited to a max 30 day supply and require a prior authorization (copay amount listed below) Tier 1 – Generic $10 / $25 copay Not Applicable (Retail/Mail Order) Tier 2 - Preferred Brand $75 / $187.50 copay Not Applicable (Retail/Mail Order) Tier 3 - Non-Preferred Brand $150 / $375 copay Not Applicable (Retail/Mail Order) Tier 4 - Specialty $400 copay Not Applicable (Retail/Mail Order) Notes: • Dependent Age Limit: to the end of the month in which the child attains age 26. • Members are encouraged to always obtain prior approval when using Out-of-Network Providers. Precertification will help the member know if the services are considered not medically necessary. Page 6 of 10
 2025 Summary HCCSC Anthem HealthSync PPO 1 Page 5 Page 7
2025 Summary HCCSC Anthem HealthSync PPO 1 Page 5 Page 7