
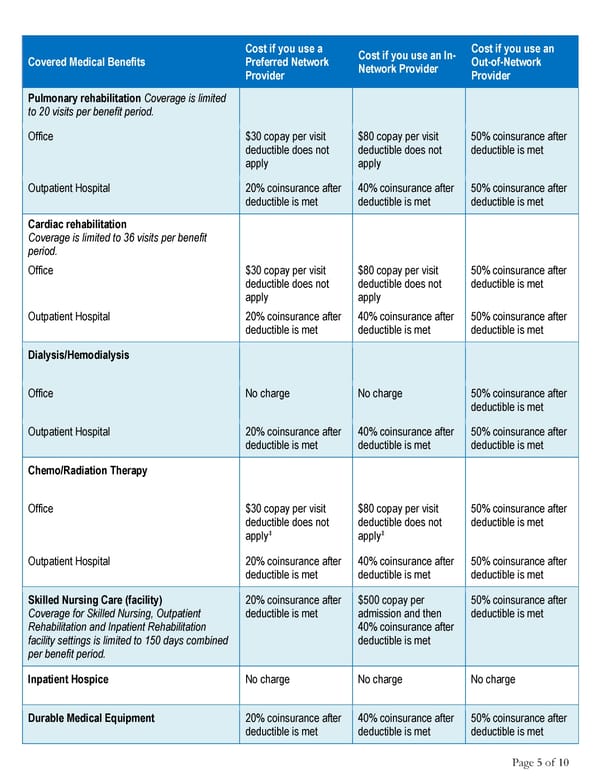
Cost if you use a Cost if you use an In- Cost if you use an Covered Medical Benefits Preferred Network Network Provider Out-of-Network Provider Provider Pulmonary rehabilitation Coverage is limited to 20 visits per benefit period. Office $30 copay per visit $80 copay per visit 50% coinsurance after deductible does not deductible does not deductible is met apply apply Outpatient Hospital 20% coinsurance after 40% coinsurance after 50% coinsurance after deductible is met deductible is met deductible is met Cardiac rehabilitation Coverage is limited to 36 visits per benefit period. Office $30 copay per visit $80 copay per visit 50% coinsurance after deductible does not deductible does not deductible is met apply apply Outpatient Hospital 20% coinsurance after 40% coinsurance after 50% coinsurance after deductible is met deductible is met deductible is met Dialysis/Hemodialysis Office No charge No charge 50% coinsurance after deductible is met Outpatient Hospital 20% coinsurance after 40% coinsurance after 50% coinsurance after deductible is met deductible is met deductible is met Chemo/Radiation Therapy Office $30 copay per visit $80 copay per visit 50% coinsurance after deductible does not deductible does not deductible is met ‡ ‡ apply apply Outpatient Hospital 20% coinsurance after 40% coinsurance after 50% coinsurance after deductible is met deductible is met deductible is met Skilled Nursing Care (facility) 20% coinsurance after $500 copay per 50% coinsurance after Coverage for Skilled Nursing, Outpatient deductible is met admission and then deductible is met Rehabilitation and Inpatient Rehabilitation 40% coinsurance after facility settings is limited to 150 days combined deductible is met per benefit period. Inpatient Hospice No charge No charge No charge Durable Medical Equipment 20% coinsurance after 40% coinsurance after 50% coinsurance after deductible is met deductible is met deductible is met Page 5 of 10
 2025 Summary HCCSC Anthem HealthSync PPO 2 Page 4 Page 6
2025 Summary HCCSC Anthem HealthSync PPO 2 Page 4 Page 6