
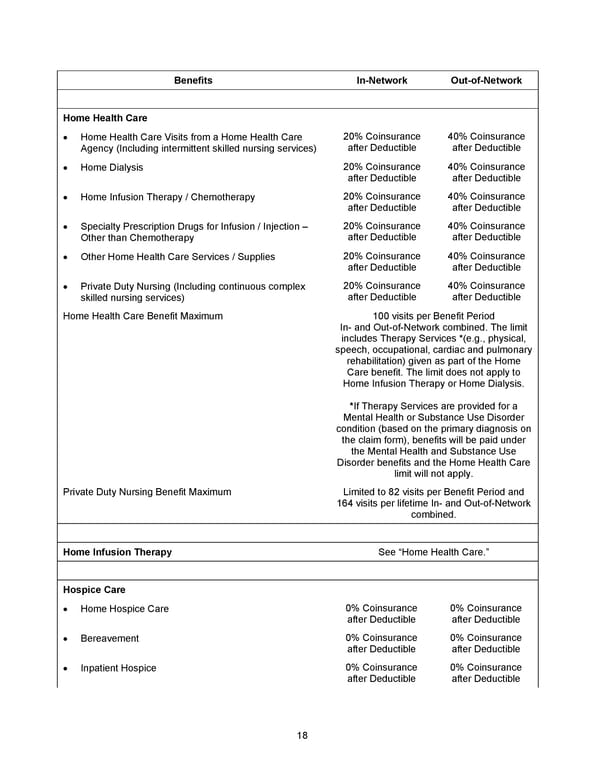
18 Benefits In - Network Out - of - Network Home Health Care • Home Health Care Visits from a Home Health Care Agency (Including intermittent skilled nursing services) 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Home Dialysis 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Home Infusion Therapy / Chemotherapy 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Specialty Prescription Drugs for Infusion / Injection – Other than Chemotherapy 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Other Home Health Care Services / Supplies 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Private Duty Nursing (Including continuous complex skilled nursing services) 20% Coinsurance after Deductible 40% Coinsurance after Deductible Home Health Care Benefit Maximum 1 0 0 visits per Benefit Period In - and Out - of - Network combined . The limit includes Therapy Services * (e.g., physical, speech, occupational , cardiac and pulmonary rehabilitation) given as part of the Home Care benefit. The limit does not apply to Home Infusion Therapy or Home Dialysis. * If Therapy Services are provided for a Mental Health or Substance Use Disorder condition (based on the primary diagnosis on the claim form) , benefits will be paid under the Mental Health and Substance Use Disorder benefits and the Home Health Care limit will not apply . Private Duty Nursing Benefit Maximum Limited to 82 visits per Benefit Period and 164 visits per lifetime In - and Out - of - Network combined . Home Infusion Therapy See “Home Health Care.” Hospice Care • Home Hospice Care 0% Coinsurance after Deductible 0% Coinsurance after Deductible • Bereavement 0% Coinsurance after Deductible 0% Coinsurance after Deductible • Inpatient Hospice 0% Coinsurance after Deductible 0% Coinsurance after Deductible
 2026 Anthem Certificate CDHP #2 Page 18 Page 20
2026 Anthem Certificate CDHP #2 Page 18 Page 20