
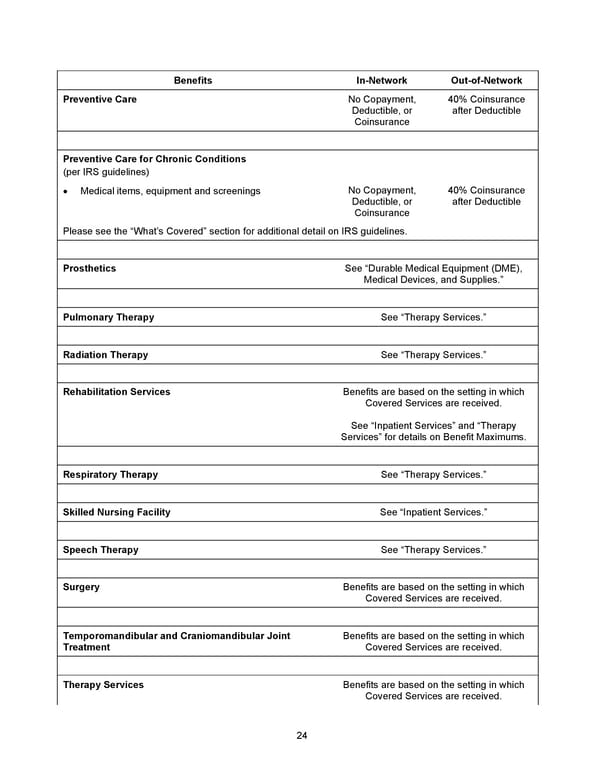
24 Benefits In - Network Out - of - Network Preventive Care No Copayment, Deductible, or Coinsurance 40% Coinsurance after Deductible Preventive Care for Chronic Conditions (per IRS guidelines) • Medical items, equipment and screenings No Copayment, Deductible, or Coinsurance 40% Coinsurance after Deductible Please see the “What’s Covered” section for additional detail on IRS guidelines. Prosthetics See “ Durable Medical Equipment (DME), Medical Devices, and Supplies. ” Pulmonary Therapy See “Therapy Services.” Radiation Therapy See “Therapy Services.” Rehabilitation Services Benefits are based on the setting in which Covered Services are received. See “Inpatient Services” and “Therapy Services” for details on Benefit Maximums. Respiratory Therapy See “Therapy Services.” Skilled Nursing Facility See “Inpatient Services.” Speech Therapy See “Therapy Services.” Surgery Benefits are based on the setting in which Covered Services are received. Temporomandibular and Craniomandibular Joint Treatment Benefits are based on the setting in which Covered Services are received . Therapy Services Benefits are based on the setting in which Covered Services are received.
 2026 Anthem Certificate CDHP #3 Page 24 Page 26
2026 Anthem Certificate CDHP #3 Page 24 Page 26