
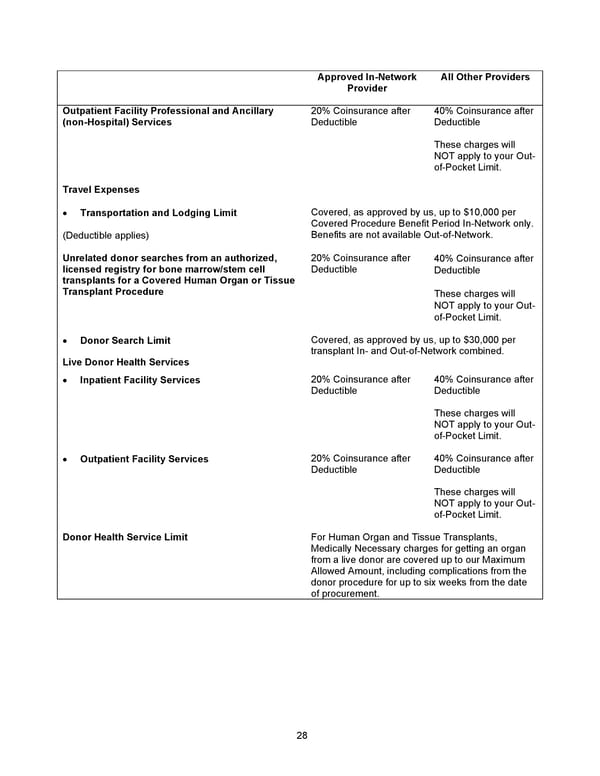
28 Approved In - Network Provider All Other Providers Outpatient Facility Professional and Ancillary (non - Hospital) Services 20% Coinsurance after Deductible 40% Coinsurance after Deductible These charges will NOT apply to y our Out - of - Pocket Limit. Travel Expenses • Transportation and Lodging Limit (Deductible applies) Covered, as approved by us, up to $10,000 per Covered Procedure Benefit Period In - Network only. Benefits are not available Out - of - Network . Unrelated donor searches from an authorized, licensed registry for bone marrow/stem cell transplants for a Covered Human Organ or Tissue Transplant Procedure 20% Coinsurance after Deductible 40% Coinsurance after Deductible These charges will NOT apply to your Out - of - Pocket Limit. • Donor Search Limit Covered, as approved by us, up to $30,000 per transplant In - and Out - of - Network combined. Live Donor Health Services • Inpatient Facility Services 20% Coinsurance after Deductible 40% Coinsurance after Deductible These charges will NOT apply to your Out - of - Pocket Limit . • Outpatient Facility Services 20% Coinsurance after Deductible 40% Coinsurance after Deductible These charges will NOT apply to your Out - of - Pocket Limit. Donor Health Service Limit For Human Organ and Tissue Transplants, Medically Necessary charges for getting an organ from a live donor are covered up to our Maximum Allowed Amount, including complications from the donor procedure for up to six weeks from the date of procurement.
 2026 Anthem Certificate CDHP #3 Page 28 Page 30
2026 Anthem Certificate CDHP #3 Page 28 Page 30