
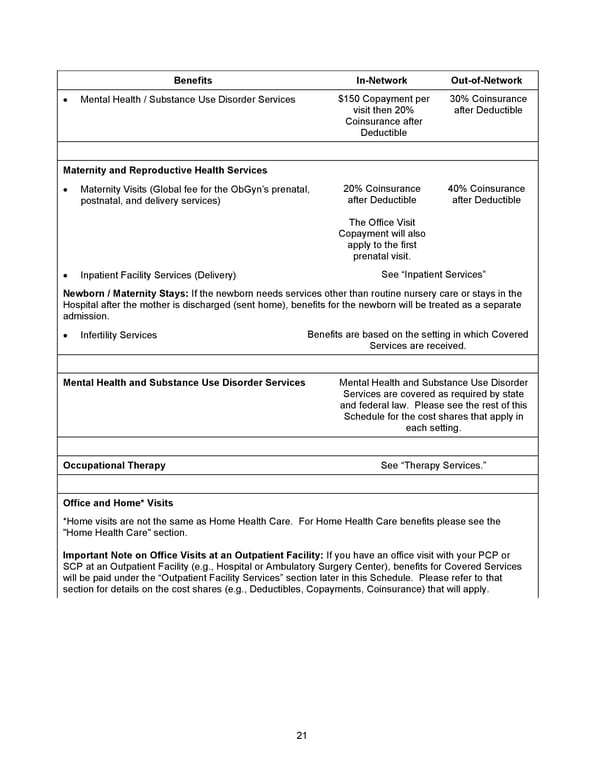
21 Benefits In - Network Out - of - Network • Mental Health / Substance Use Disorder Services $150 Copayment per visit then 20% Coinsurance after Deductible 30% Coinsurance after Deductible Maternity and Reproductive Health Services • Maternity Visits (Global fee for the ObGyn’s prenatal, postnatal, and delivery services) 20% Coinsurance after Deductible The Office Visit Copayment will also apply to the first prenatal visit. 40% Coinsurance after Deductible • Inpatient Facility Services (Delivery) See “Inpatient Services” Newborn / Maternity Stays: If the newborn needs services other than routine nursery care or stays in the Hospital after the mother is discharged (sent home), benefits for the newborn will be treated as a separate admission. • Infertility Services Benefits are based on the setting in which Covered Services are received. Mental Health and Substance Use Disorder Services Mental Health and Substance Use Disorder Services are covered as required by state and federal law. Please see the rest of this Schedule for the cost shares that apply in each setting. Occupational Therapy See “Therapy Services.” Office and Home* Visits *Home visits are not the same as Home Health Care. For Home Health Care benefits please see the "Home Health Care" section. Important Note on Office Visits at an Outpatient Facility: If you have an office visit with your PCP or SCP at an Outpatient Facility (e.g., Hospital or Ambulatory Surgery Center), benefits for Covered Services will be paid under the “Outpatient Facility Services” section later in this Schedule. Please refer to that section for details on the cost shares (e.g., Deductibles, Copayments, Coinsurance) that will apply.
 2026 Anthem Certificate Plan B Page 21 Page 23
2026 Anthem Certificate Plan B Page 21 Page 23