
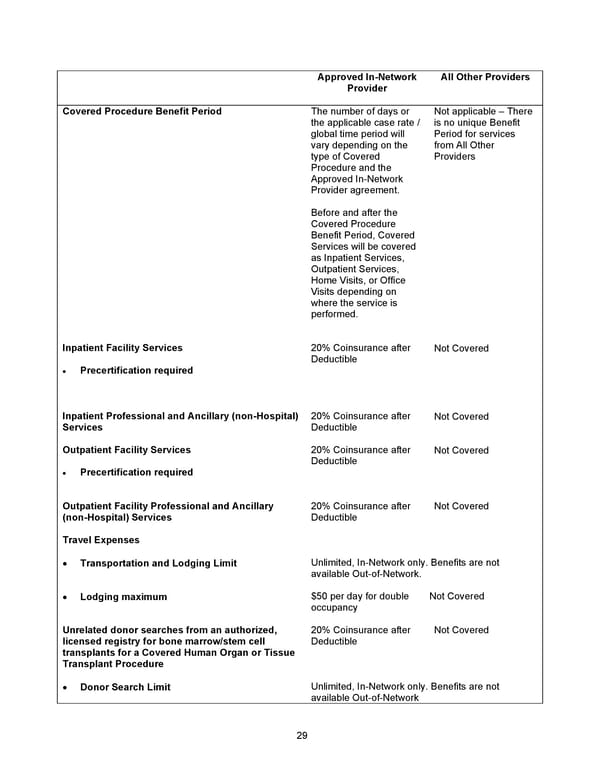
29 Approved In - Network Provider All Other Providers Covered Procedure Benefit Period The number of days or the applicable case rate / global time period will vary depending on the type of Covered Procedure and the Approved In - Network Provider agreement. Before and after the Covered Procedure Benefit Period, Covered Services will be covered as Inpatient Services, Outpatient Services, Home Visits, or Office Visits depending on where the service is performed. Not applicable – There is no unique Benefit Period for services from All Other Providers Inpatient Facility Services • Precertification required 20% Coinsurance after Deductible Not Covered Inpatient Professional and Ancillary (non - Hospital) Services 20% Coinsurance after Deductible Not Covered Outpatient Facility Services • Precertification required 20% Coinsurance after Deductible Not Covered Outpatient Facility Professional and Ancillary (non - Hospital) Services 20% Coinsurance after Deductible Not Covered Travel Expenses • Transportation and Lodging Limit Unlimited, In - Network only. Benefits are not available Out - of - Network . • Lodging maximum $50 per day for double occupancy Not Covered Unrelated donor searches from an authorized, licensed registry for bone marrow/stem cell transplants for a Covered Human Organ or Tissue Transplant Procedure 20% Coinsurance after Deductible Not Covered • Donor Search Limit Unlimited, In - Network only. Benefits are not available Out - of - Network
 2026 Anthem Certificate Plan B Page 29 Page 31
2026 Anthem Certificate Plan B Page 29 Page 31