
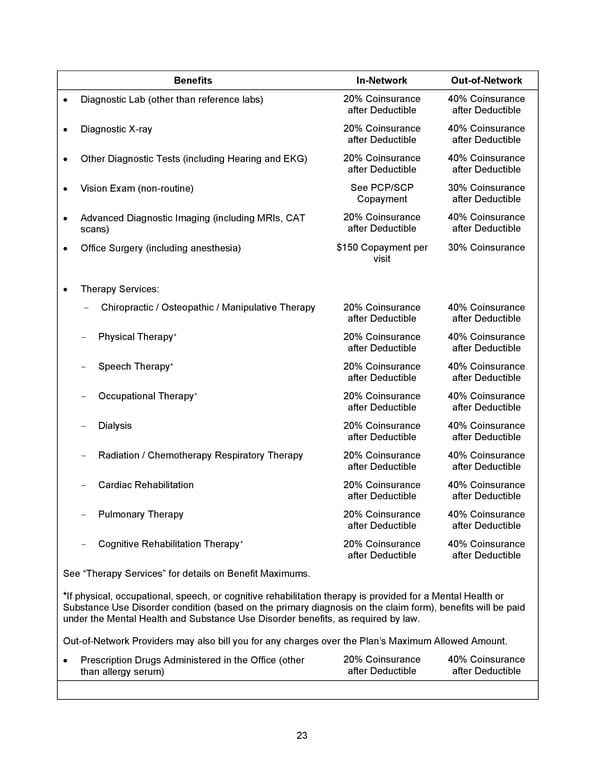
23 Benefits In - Network Out - of - Network • Diagnostic Lab (other than reference labs) 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Diagnostic X - ray 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Other Diagnostic Tests (including Hearing and EKG) 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Vision Exam (non - routine) See PCP/SCP Copayment 3 0 % Coinsurance after Deductible • Advanced Diagnostic Imaging (including MRIs, CAT scans) 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Office Surgery (including anesthesia) $150 Copayment per visit 3 0% Coinsurance • Therapy Services: - Chiropractic / Osteopathic / Manipulative Therapy 20% Coinsurance after Deductible 40% Coinsurance after Deductible - Physical Therapy + 20% Coinsurance after Deductible 40% Coinsurance after Deductible - Speech Therapy + 20% Coinsurance after Deductible 40% Coinsurance after Deductible - Occupational Therapy + 20% Coinsurance after Deductible 40% Coinsurance after Deductible - Dialysis 20% Coinsurance after Deductible 40% Coinsurance after Deductible - Radiation / Chemotherapy Respiratory Therapy 20% Coinsurance after Deductible 40% Coinsurance after Deductible - Cardiac Rehabilitation 20% Coinsurance after Deductible 40% Coinsurance after Deductible - Pulmonary Therapy 20% Coinsurance after Deductible 40% Coinsurance after Deductible - Cognitive Rehabilitation Therapy + 20% Coinsurance after Deductible 40% Coinsurance after Deductible See “Therapy Services” for details on Benefit Maximums. + If physical, occupational, speech, or cognitive rehabilitation therapy is provided for a Mental Health or Substance Use Disorder condition (based on the primary diagnosis on the claim form), benefits will be paid under the Mental Health and Substance Use D isorder benefits, as required by law. Out - of - Network Providers may also bill you for any charges over the Plan’s Maximum Allowed Amount. • Prescription Drugs Administered in the Office (other than allergy serum) 20% Coinsurance after Deductible 40% Coinsurance after Deductible
 2026 Anthem Certificate Plan B Page 23 Page 25
2026 Anthem Certificate Plan B Page 23 Page 25