
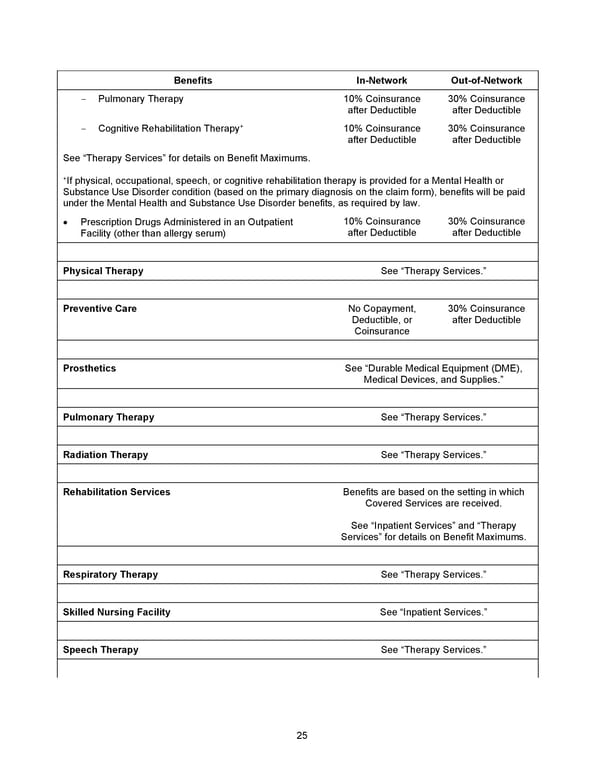
25 Benefits In - Network Out - of - Network - Pulmonary Therapy 10% Coinsurance after Deductible 30% Coinsurance after Deductible - Cognitive Rehabilitation Therapy + 10% Coinsurance after Deductible 30% Coinsurance after Deductible See “Therapy Services” for details on Benefit Maximums. + If physical, occupational, speech, or cognitive rehabilitation therapy is provided for a Mental Health or Substance Use Disorder condition (based on the primary diagnosis on the claim form), benefits will be paid under the Mental Health and Substance Use D isorder benefits, as required by law. • Prescription Drugs Administered in an Outpatient Facility (other than allergy serum) 10% Coinsurance after Deductible 30% Coinsurance after Deductible Physical Therapy See “Therapy Services.” Preventive Care No Copayment, Deductible, or Coinsurance 30% Coinsurance after Deductible Prosthetics See “ Durable Medical Equipment (DME), Medical Devices, and Supplies. ” Pulmonary Therapy See “Therapy Services.” Radiation Therapy See “Therapy Services.” Rehabilitation Services Benefits are based on the setting in which Covered Services are received. See “Inpatient Services” and “Therapy Services” for details on Benefit Maximums. Respiratory Therapy See “Therapy Services.” Skilled Nursing Facility See “Inpatient Services.” Speech Therapy See “Therapy Services.”
 2026 Anthem Certificate Plan C Page 25 Page 27
2026 Anthem Certificate Plan C Page 25 Page 27