
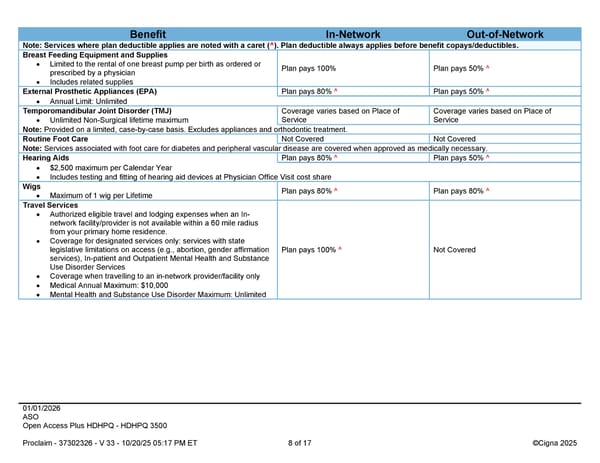
01/01/2026 ASO Open Access Plus HDHPQ - HDHPQ 3500 Proclaim - 37302326 - V 33 - 10/20/25 05:17 PM ET 8 of 17 ©Cigna 2025 Benefit In-Network Out-of-Network Note: Services where plan deductible applies are noted with a caret (^). Plan deductible always applies before benefit copays/deductibles. Breast Feeding Equipment and Supplies Limited to the rental of one breast pump per birth as ordered or prescribed by a physician Includes related supplies Plan pays 100% Plan pays 50% ^ External Prosthetic Appliances (EPA) Plan pays 80% ^ Plan pays 50% ^ Annual Limit: Unlimited Temporomandibular Joint Disorder (TMJ) Unlimited Non-Surgical lifetime maximum Coverage varies based on Place of Service Coverage varies based on Place of Service Note: Provided on a limited, case-by-case basis. Excludes appliances and orthodontic treatment. Routine Foot Care Not Covered Not Covered Note: Services associated with foot care for diabetes and peripheral vascular disease are covered when approved as medically necessary. Hearing Aids Plan pays 80% ^ Plan pays 50% ^ $2,500 maximum per Calendar Year Includes testing and fitting of hearing aid devices at Physician Office Visit cost share Wigs Maximum of 1 wig per Lifetime Plan pays 80% ^ Plan pays 80% ^ Travel Services Authorized eligible travel and lodging expenses when an In- network facility/provider is not available within a 60 mile radius from your primary home residence. Coverage for designated services only: services with state legislative limitations on access (e.g., abortion, gender affirmation services), In-patient and Outpatient Mental Health and Substance Use Disorder Services Coverage when travelling to an in-network provider/facility only Medical Annual Maximum: $10,000 Mental Health and Substance Use Disorder Maximum: Unlimited Plan pays 100% ^ Not Covered
 2026 Cigna Health Plan Benefit Summary HDHP 3500 Page 7 Page 9
2026 Cigna Health Plan Benefit Summary HDHP 3500 Page 7 Page 9