
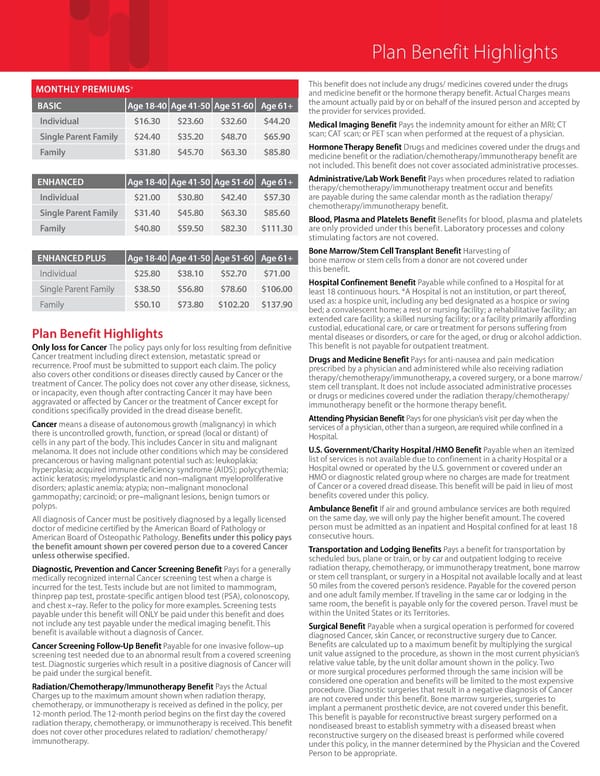
Plan Benefit Highlights Only loss for Cancer The policy pays only for loss resulting from definitive Cancer treatment including direct extension, metastatic spread or recurrence. Proof must be submitted to support each claim. The policy also covers other conditions or diseases directly caused by Cancer or the treatment of Cancer. The policy does not cover any other disease, sickness, or incapacity, even though after contracting Cancer it may have been aggravated or affected by Cancer or the treatment of Cancer except for conditions specifically provided in the dread disease benefit. Cancer means a disease of autonomous growth (malignancy) in which there is uncontrolled growth, function, or spread (local or distant) of cells in any part of the body. This includes Cancer in situ and malignant melanoma. It does not include other conditions which may be considered precancerous or having malignant potential such as: leukoplakia; hyperplasia; acquired immune deficiency syndrome (AIDS); polycythemia; actinic keratosis; myelodysplastic and non–malignant myeloproliferative disorders; aplastic anemia; atypia; non–malignant monoclonal gammopathy; carcinoid; or pre–malignant lesions, benign tumors or polyps. All diagnosis of Cancer must be positively diagnosed by a legally licensed doctor of medicine certified by the American Board of Pathology or American Board of Osteopathic Pathology. Benefits under this policy pays the benefit amount shown per covered person due to a covered Cancer unless otherwise specified. Diagnostic, Prevention and Cancer Screening Benefit Pays for a generally medically recognized internal Cancer screening test when a charge is incurred for the test. Tests include but are not limited to mammogram, thinprep pap test, prostate-specific antigen blood test (PSA), colonoscopy, and chest x–ray. Refer to the policy for more examples. Screening tests payable under this benefit will ONLY be paid under this benefit and does not include any test payable under the medical imaging benefit. This benefit is available without a diagnosis of Cancer. Cancer Screening Follow-Up Benefit Payable for one invasive follow–up screening test needed due to an abnormal result from a covered screening test. Diagnostic surgeries which result in a positive diagnosis of Cancer will be paid under the surgical benefit. Radiation/Chemotherapy/Immunotherapy Benefit Pays the Actual Charges up to the maximum amount shown when radiation therapy, chemotherapy, or immunotherapy is received as defined in the policy, per 12-month period. The 12-month period begins on the first day the covered radiation therapy, chemotherapy, or immunotherapy is received. This benefit does not cover other procedures related to radiation/ chemotherapy/ immunotherapy. This benefit does not include any drugs/ medicines covered under the drugs and medicine benefit or the hormone therapy benefit. Actual Charges means the amount actually paid by or on behalf of the insured person and accepted by the provider for services provided. Medical Imaging Benefit Pays the indemnity amount for either an MRI; CT scan; CAT scan; or PET scan when performed at the request of a physician. Hormone Therapy Benefit Drugs and medicines covered under the drugs and medicine benefit or the radiation/chemotherapy/immunotherapy benefit are not included. This benefit does not cover associated administrative processes. Administrative/Lab Work Benefit Pays when procedures related to radiation therapy/chemotherapy/immunotherapy treatment occur and benefits are payable during the same calendar month as the radiation therapy/ chemotherapy/immunotherapy benefit. Blood, Plasma and Platelets Benefit Benefits for blood, plasma and platelets are only provided under this benefit. Laboratory processes and colony stimulating factors are not covered. Bone Marrow/Stem Cell Transplant Benefit Harvesting of bone marrow or stem cells from a donor are not covered under this benefit. Hospital Confinement Benefit Payable while confined to a Hospital for at least 18 continuous hours. *A Hospital is not an institution, or part thereof, used as: a hospice unit, including any bed designated as a hospice or swing bed; a convalescent home; a rest or nursing facility; a rehabilitative facility; an extended care facility; a skilled nursing facility; or a facility primarily affording custodial, educational care, or care or treatment for persons suffering from mental diseases or disorders, or care for the aged, or drug or alcohol addiction. This benefit is not payable for outpatient treatment. Drugs and Medicine Benefit Pays for anti-nausea and pain medication prescribed by a physician and administered while also receiving radiation therapy/chemotherapy/immunotherapy, a covered surgery, or a bone marrow/ stem cell transplant. It does not include associated administrative processes or drugs or medicines covered under the radiation therapy/chemotherapy/ immunotherapy benefit or the hormone therapy benefit. Attending Physician Benefit Pays for one physician’s visit per day when the services of a physician, other than a surgeon, are required while confined in a Hospital. U.S. Government/Charity Hospital /HMO Benefit Payable when an itemized list of services is not available due to confinement in a charity Hospital or a Hospital owned or operated by the U.S. government or covered under an HMO or diagnostic related group where no charges are made for treatment of Cancer or a covered dread disease. This benefit will be paid in lieu of most benefits covered under this policy. Ambulance Benefit If air and ground ambulance services are both required on the same day, we will only pay the higher benefit amount. The covered person must be admitted as an inpatient and Hospital confined for at least 18 consecutive hours. Transportation and Lodging Benefits Pays a benefit for transportation by scheduled bus, plane or train, or by car and outpatient lodging to receive radiation therapy, chemotherapy, or immunotherapy treatment, bone marrow or stem cell transplant, or surgery in a Hospital not available locally and at least 50 miles from the covered person’s residence. Payable for the covered person and one adult family member. If traveling in the same car or lodging in the same room, the benefit is payable only for the covered person. Travel must be within the United States or its Territories. Surgical Benefit Payable when a surgical operation is performed for covered diagnosed Cancer, skin Cancer, or reconstructive surgery due to Cancer. Benefits are calculated up to a maximum benefit by multiplying the surgical unit value assigned to the procedure, as shown in the most current physician’s relative value table, by the unit dollar amount shown in the policy. Two or more surgical procedures performed through the same incision will be considered one operation and benefits will be limited to the most expensive procedure. Diagnostic surgeries that result in a negative diagnosis of Cancer are not covered under this benefit. Bone marrow surgeries, surgeries to implant a permanent prosthetic device, are not covered under this benefit. This benefit is payable for reconstructive breast surgery performed on a nondiseased breast to establish symmetry with a diseased breast when reconstructive surgery on the diseased breast is performed while covered under this policy, in the manner determined by the Physician and the Covered Person to be appropriate. Plan Benefit Highlights MONTHLY PREMIUMS+ BASIC Age 18-40 Age 41-50 Age 51-60 Age 61+ Individual $16.30 $23.60 $32.60 $44.20 Single Parent Family $24.40 $35.20 $48.70 $65.90 Family $31.80 $45.70 $63.30 $85.80 ENHANCED Age 18-40 Age 41-50 Age 51-60 Age 61+ Individual $21.00 $30.80 $42.40 $57.30 Single Parent Family $31.40 $45.80 $63.30 $85.60 Family $40.80 $59.50 $82.30 $111.30 ENHANCED PLUS Age 18-40 Age 41-50 Age 51-60 Age 61+ Individual $25.80 $38.10 $52.70 $71.00 Single Parent Family $38.50 $56.80 $78.60 $106.00 Family $50.10 $73.80 $102.20 $137.90
 American Fidelity Individual Cancer Insurance Overview Page 2 Page 4
American Fidelity Individual Cancer Insurance Overview Page 2 Page 4