
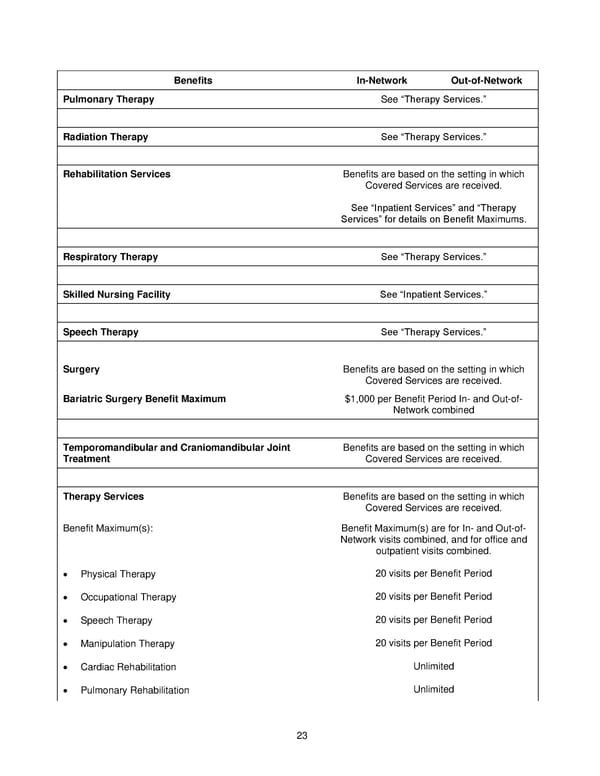
23 Benefits In-Network Out-of-Network Pulmonary Therapy See “Therapy Services.” Radiation Therapy See “Therapy Services.” Rehabilitation Services Benefits are based on the setting in which Covered Services are received. See “Inpatient Services” and “Therapy Services” for details on Benefit Maximums. Respiratory Therapy See “Therapy Services.” Skilled Nursing Facility See “Inpatient Services.” Speech Therapy See “Therapy Services.” Surgery Benefits are based on the setting in which Covered Services are received. Bariatric Surgery Benefit Maximum $1,000 per Benefit Period In- and Out-of- Network combined Temporomandibular and Craniomandibular Joint Treatment Benefits are based on the setting in which Covered Services are received. Therapy Services Benefits are based on the setting in which Covered Services are received. Benefit Maximum(s): Benefit Maximum(s) are for In- and Out-of- Network visits combined, and for office and outpatient visits combined. • Physical Therapy 20 visits per Benefit Period • Occupational Therapy 20 visits per Benefit Period • Speech Therapy 20 visits per Benefit Period • Manipulation Therapy 20 visits per Benefit Period • Cardiac Rehabilitation Unlimited • Pulmonary Rehabilitation Unlimited
 Anthem Blue Access PPO HSA Option E6 IN PPO Large 96R6 01 01 2025 L12026MR02 L12026 English EOC CY Page 23 Page 25
Anthem Blue Access PPO HSA Option E6 IN PPO Large 96R6 01 01 2025 L12026MR02 L12026 English EOC CY Page 23 Page 25