
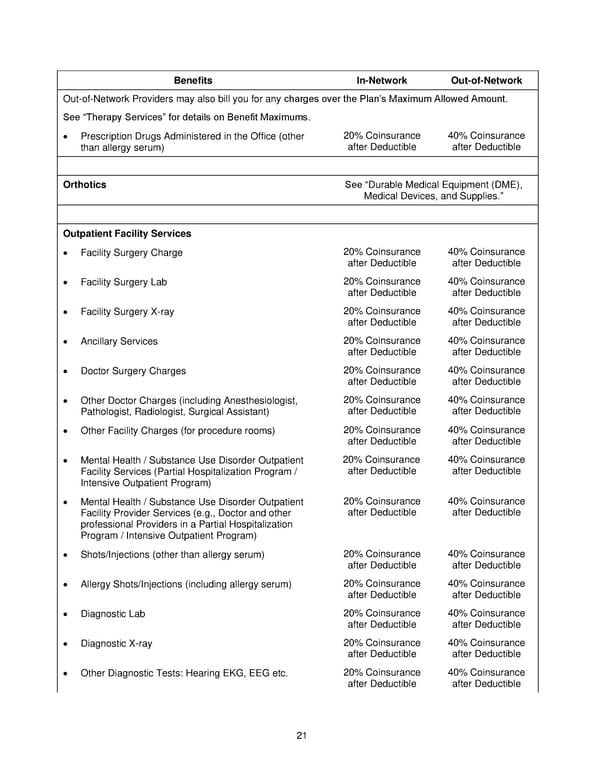
21 Benefits In-Network Out-of-Network Out-of-Network Providers may also bill you for any charges over the Plan’s Maximum Allowed Amount. See “Therapy Services” for details on Benefit Maximums. • Prescription Drugs Administered in the Office (other than allergy serum) 20% Coinsurance after Deductible 40% Coinsurance after Deductible Orthotics See “Durable Medical Equipment (DME), Medical Devices, and Supplies.” Outpatient Facility Services • Facility Surgery Charge 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Facility Surgery Lab 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Facility Surgery X-ray 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Ancillary Services 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Doctor Surgery Charges 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Other Doctor Charges (including Anesthesiologist, Pathologist, Radiologist, Surgical Assistant) 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Other Facility Charges (for procedure rooms) 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Mental Health / Substance Use Disorder Outpatient Facility Services (Partial Hospitalization Program / Intensive Outpatient Program) 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Mental Health / Substance Use Disorder Outpatient Facility Provider Services (e.g., Doctor and other professional Providers in a Partial Hospitalization Program / Intensive Outpatient Program) 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Shots/Injections (other than allergy serum) 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Allergy Shots/Injections (including allergy serum) 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Diagnostic Lab 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Diagnostic X-ray 20% Coinsurance after Deductible 40% Coinsurance after Deductible • Other Diagnostic Tests: Hearing EKG, EEG etc. 20% Coinsurance after Deductible 40% Coinsurance after Deductible
 Anthem Blue Access PPO HSA Option E6 IN PPO Large 96R6 01 01 2025 L12026MR02 L12026 English EOC CY Page 21 Page 23
Anthem Blue Access PPO HSA Option E6 IN PPO Large 96R6 01 01 2025 L12026MR02 L12026 English EOC CY Page 21 Page 23