
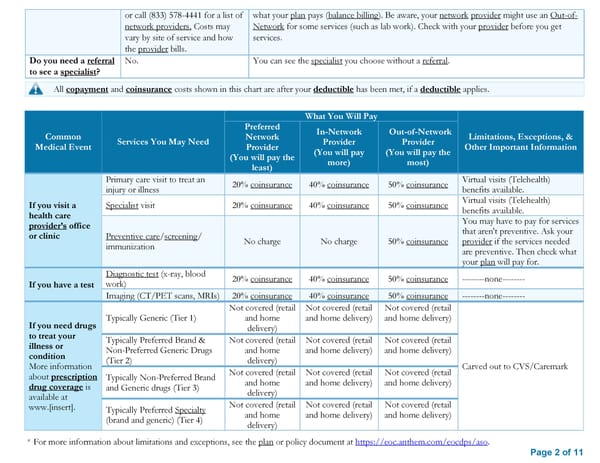
or call (833) 578-4441 for a list of what your plan pays (balance billing). Be aware, your network provider might use an Out-of- network providers. Costs may Network for some services (such as lab work). Check with your provider before you get vary by site of service and how services. the provider bills. Do you need a referral No. You can see the specialist you choose without a referral. to see a specialist? All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies. What You Will Pay Preferred In-Network Out-of-Network Common Services You May Need Network Provider Provider Limitations, Exceptions, & Medical Event Provider (You will pay (You will pay the Other Important Information (You will pay the more) most) least) Primary care visit to treat an 20% coinsurance 40% coinsurance 50% coinsurance Virtual visits (Telehealth) injury or illness benefits available. If you visit a Specialist visit 20% coinsurance 40% coinsurance 50% coinsurance Virtual visits (Telehealth) health care benefits available. provider’s office You may have to pay for services or clinic Preventive care/screening/ that aren't preventive. Ask your immunization No charge No charge 50% coinsurance provider if the services needed are preventive. Then check what your plan will pay for. Diagnostic test (x-ray, blood 20% coinsurance 40% coinsurance 50% coinsurance --------none-------- If you have a test work) Imaging (CT/PET scans, MRIs) 20% coinsurance 40% coinsurance 50% coinsurance --------none-------- Not covered (retail Not covered (retail Not covered (retail If you need drugs Typically Generic (Tier 1) and home and home delivery) and home delivery) to treat your delivery) illness or Typically Preferred Brand & Not covered (retail Not covered (retail Not covered (retail condition Non-Preferred Generic Drugs and home and home delivery) and home delivery) More information (Tier 2) delivery) Carved out to CVS/Caremark about prescription Typically Non-Preferred Brand Not covered (retail Not covered (retail Not covered (retail drug coverage is and Generic drugs (Tier 3) and home and home delivery) and home delivery) available at delivery) www.[insert]. Typically Preferred Specialty Not covered (retail Not covered (retail Not covered (retail (brand and generic) (Tier 4) and home and home delivery) and home delivery) delivery) * For more information about limitations and exceptions, see the plan or policy document at https://eoc.anthem.com/eocdps/aso. Page 2 of 11
 Anthem SBC Option 2 Page 1 Page 3
Anthem SBC Option 2 Page 1 Page 3