
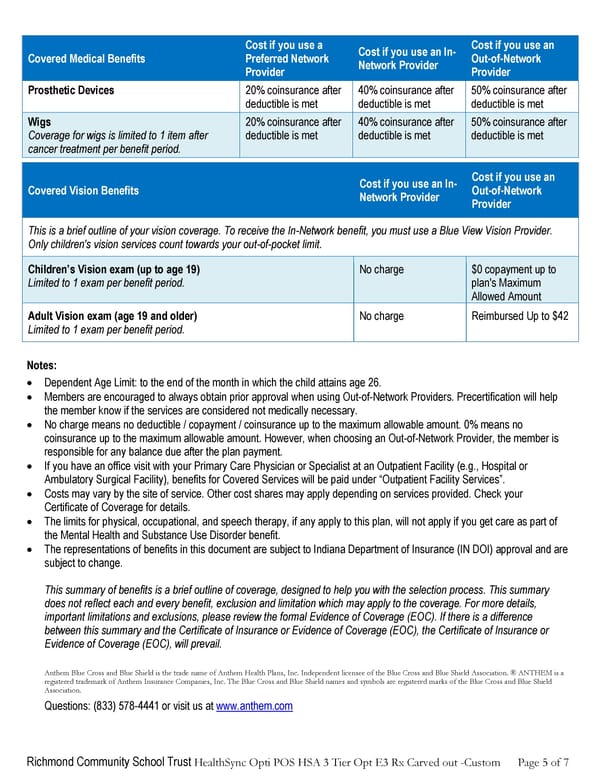
Richmond Community School Trust HealthSync Opti POS HSA 3 Tier Opt E3 Rx Carved out -Custom Page 5 of 7 Covered Medical Benefits Cost if you use a Preferred Network Provider Cost if you use an In- Network Provider Cost if you use an Out-of-Network Provider Prosthetic Devices 20% coinsurance after deductible is met 40% coinsurance after deductible is met 50% coinsurance after deductible is met Wigs Coverage for wigs is limited to 1 item after cancer treatment per benefit period. 20% coinsurance after deductible is met 40% coinsurance after deductible is met 50% coinsurance after deductible is met Covered Vision Benefits Cost if you use an In- Network Provider Cost if you use an Out-of-Network Provider This is a brief outline of your vision coverage. To receive the In-Network benefit, you must use a Blue View Vision Provider. Only children's vision services count towards your out-of-pocket limit. Children’s Vision exam (up to age 19) Limited to 1 exam per benefit period. No charge $0 copayment up to plan's Maximum Allowed Amount Adult Vision exam (age 19 and older) Limited to 1 exam per benefit period. No charge Reimbursed Up to $42 Notes: • Dependent Age Limit: to the end of the month in which the child attains age 26. • Members are encouraged to always obtain prior approval when using Out-of-Network Providers. Precertification will help the member know if the services are considered not medically necessary. • No charge means no deductible / copayment / coinsurance up to the maximum allowable amount. 0% means no coinsurance up to the maximum allowable amount. However, when choosing an Out-of-Network Provider, the member is responsible for any balance due after the plan payment. • If you have an office visit with your Primary Care Physician or Specialist at an Outpatient Facility (e.g., Hospital or Ambulatory Surgical Facility), benefits for Covered Services will be paid under “Outpatient Facility Services”. • Costs may vary by the site of service. Other cost shares may apply depending on services provided. Check your Certificate of Coverage for details. • The limits for physical, occupational, and speech therapy, if any apply to this plan, will not apply if you get care as part of the Mental Health and Substance Use Disorder benefit. • The representations of benefits in this document are subject to Indiana Department of Insurance (IN DOI) approval and are subject to change. This summary of benefits is a brief outline of coverage, designed to help you with the selection process. This summary does not reflect each and every benefit, exclusion and limitation which may apply to the coverage. For more details, important limitations and exclusions, please review the formal Evidence of Coverage (EOC). If there is a difference between this summary and the Certificate of Insurance or Evidence of Coverage (EOC), the Certificate of Insurance or Evidence of Coverage (EOC), will prevail. Anthem Blue Cross and Blue Shield is the trade name of Anthem Health Plans, Inc. Independent licensee of the Blue Cross and Blue Shield Association. ® ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. The Blue Cross and Blue Shield names and symbols are registered marks of the Blue Cross and Blue Shield Association. Questions: (833) 578-4441 or visit us at www.anthem.com
 Anthem Summary of Benefits HDHP 2 Page 4 Page 6
Anthem Summary of Benefits HDHP 2 Page 4 Page 6