
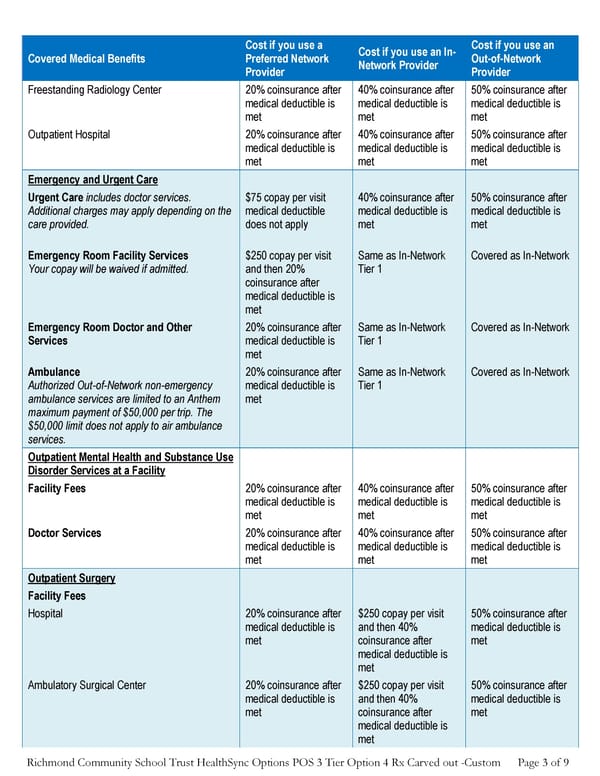
Richmond Community School Trust HealthSync Options POS 3 Tier Option 4 Rx Carved out -Custom Page 3 of 9 Covered Medical Benefits Cost if you use a Preferred Network Provider Cost if you use an In- Network Provider Cost if you use an Out-of-Network Provider Freestanding Radiology Center 20% coinsurance after medical deductible is met 40% coinsurance after medical deductible is met 50% coinsurance after medical deductible is met Outpatient Hospital 20% coinsurance after medical deductible is met 40% coinsurance after medical deductible is met 50% coinsurance after medical deductible is met Emergency and Urgent Care Urgent Care includes doctor services. Additional charges may apply depending on the care provided. $75 copay per visit medical deductible does not apply 40% coinsurance after medical deductible is met 50% coinsurance after medical deductible is met Emergency Room Facility Services Your copay will be waived if admitted. $250 copay per visit and then 20% coinsurance after medical deductible is met Same as In-Network Tier 1 Covered as In-Network Emergency Room Doctor and Other Services 20% coinsurance after medical deductible is met Same as In-Network Tier 1 Covered as In-Network Ambulance Authorized Out-of-Network non-emergency ambulance services are limited to an Anthem maximum payment of $50,000 per trip. The $50,000 limit does not apply to air ambulance services. 20% coinsurance after medical deductible is met Same as In-Network Tier 1 Covered as In-Network Outpatient Mental Health and Substance Use Disorder Services at a Facility Facility Fees 20% coinsurance after medical deductible is met 40% coinsurance after medical deductible is met 50% coinsurance after medical deductible is met Doctor Services 20% coinsurance after medical deductible is met 40% coinsurance after medical deductible is met 50% coinsurance after medical deductible is met Outpatient Surgery Facility Fees Hospital 20% coinsurance after medical deductible is met $250 copay per visit and then 40% coinsurance after medical deductible is met 50% coinsurance after medical deductible is met Ambulatory Surgical Center 20% coinsurance after medical deductible is met $250 copay per visit and then 40% coinsurance after medical deductible is met 50% coinsurance after medical deductible is met
 Anthem Summary of Benefits PPO Plan Page 2 Page 4
Anthem Summary of Benefits PPO Plan Page 2 Page 4