
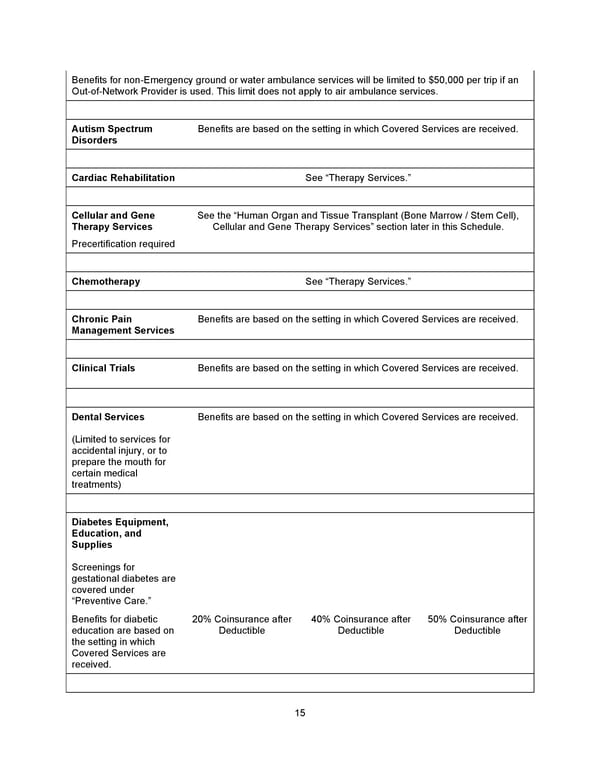
15 Benefits for non - Emergency ground or water ambulance services will be limited to $50,000 per trip if an Out - of - Network Provider is used. This limit does not apply to air ambulance services. Autism Spectrum Disorders Benefits are based on the setting in which Covered Services are received. Cardiac Rehabilitation See “Therapy Services.” Cellular and Gene Therapy Services Precertification required See the “Human Organ and Tissue Transplant (Bone Marrow / Stem Cell), Cellular and Gene Therapy Services” section later in this Schedule. Chemotherapy See “Therapy Services.” Chronic Pain Management Services Benefits are based on the setting in which Covered Services are received. Clinical Trials Benefits are based on the setting in which Covered Services are received. Dental Services (Limited to services for accidental injury, or to prepare the mouth for certain medical treatmen ts) Benefits are based on the setting in which Covered Services are received. Diabetes Equipment, Education, and Supplies Screenings for gestational diabetes are covered under “Preventive Car e.” Benefits for diabetic education are based on the setting in which Covered Services are received. 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible
 Benefit Booklet: Plan 1 Page 15 Page 17
Benefit Booklet: Plan 1 Page 15 Page 17