
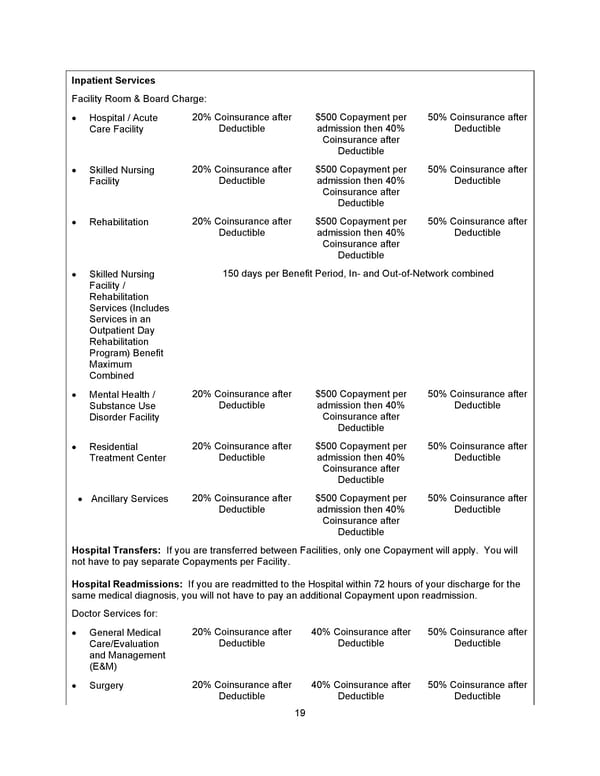
19 Inpatient Services Facility Room & Board Charge: • Hospital / Acute Care Facility 20% Coinsurance after Deductible $500 Copayment per admission then 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Skilled Nursing Facility 20% Coinsurance after Deductible $500 Copayment per admission then 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Rehabilitation 20% Coinsurance after Deductible $500 Copayment per admission then 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Skilled Nursing Facility / Rehabilitation Services (Includes Services in an Outpatient Day Rehabilitation Program) Benefit Maximum Combined 1 5 0 days per Benefit Period, In - and Out - of - Network combined • Mental Health / Substance Use Disorder Facility 20% Coinsurance after Deductible $500 Copayment per admission then 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Residential Treatment Center 20% Coinsurance after Deductible $500 Copayment per admission then 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Ancillary Services 20% Coinsurance after Deductible $500 Copayment per admission then 40% Coinsurance after Deductible 50% Coinsurance after Deductible Hospital Transfers: If you are transferred between Facilities, only one Copayment will apply. You will not have to pay separate Copayments per Facility . Hospital Readmissions: If you are readmitted to the Hospital within 72 hours of your discharge for the same medical diagnosis, you will not have to pay an additional Copayment upon readmission. Doctor Services for : • General Medical Care/Evaluation and Management (E&M) 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Surgery 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible
 Benefit Booklet: Plan 1 Page 19 Page 21
Benefit Booklet: Plan 1 Page 19 Page 21