
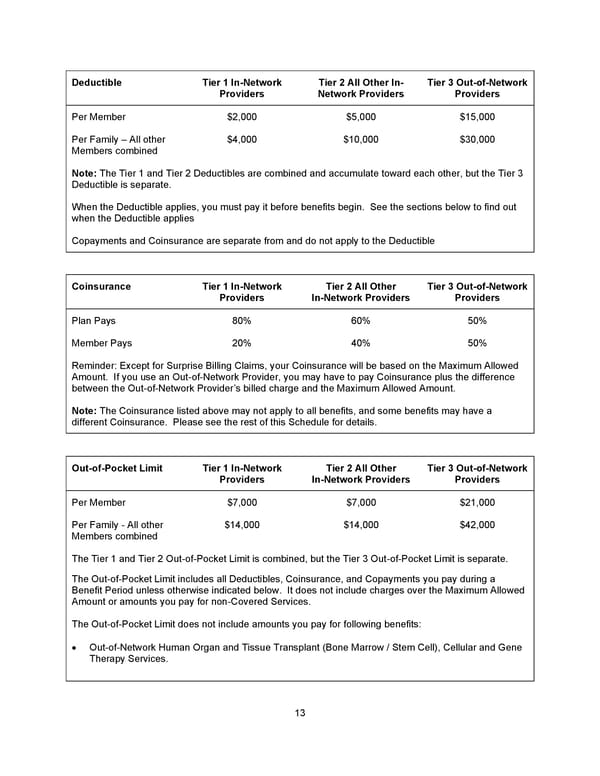
13 D eductible Tier 1 In - Network Providers Tier 2 All Other In - Network Providers Tier 3 Out - of - Network Providers Per Member $2,000 $5,000 $15,000 Per Family – All other Members combined $4,000 $10,000 $30,000 Note: The Tier 1 and Tier 2 Deductibles are combined and accumulate toward each other, but the Tier 3 Deductible is separate. When the Deductible applies, you must pay it before benefits begin. See the sections below to find out when the Deductible applies Copayments and Coinsurance are separate from and do not apply to the Deductible Coinsurance Tier 1 In - Network Providers Tier 2 All Other In - Network Providers Tier 3 Out - of - Network Providers Plan Pays 80% 60% 50% Member Pays 20% 40% 50% Reminder : Except for Surprise Billing Claims, y our Coinsurance will be based on the Maximum Allowed Amount. I f you use an Out - of - Network Provider, you may have to pay Coinsurance plus the difference between the Out - of - Network Provider’s billed charge and the Maximum Allowed Amount. Note: The Coinsurance listed above may not apply to all benefits, and some benefits may have a different Coinsurance. Please see the rest of this Schedule for details. Out - of - Pocket Limit Tier 1 In - Network Providers Tier 2 All Other In - Network Providers Tier 3 Out - of - Network Providers Per Member $7,000 $7,000 $21,000 Per Family - All other Members combined $14,000 $14,000 $42,000 The Tier 1 and Tier 2 Out - of - Pocket Limit is combined, but the Tier 3 Out - of - Pocket Limit is separate. The Out - of - Pocket Limit includes all Deductibles, Coinsurance, and Copayments you pay during a Benefit Period unless otherwise indicated below. It does not include charges over the Maximum Allowed Amount or amounts you pay for non - Covered Services. The Out - of - Pocket Limit does not include amounts you pay for following benefits: • Out - of - Network Human Organ and Tissue Transplant (Bone Marrow / Stem Cell), Cellular and Gene Therapy Services .
 Benefit Booklet: Plan 1 Page 13 Page 15
Benefit Booklet: Plan 1 Page 13 Page 15