
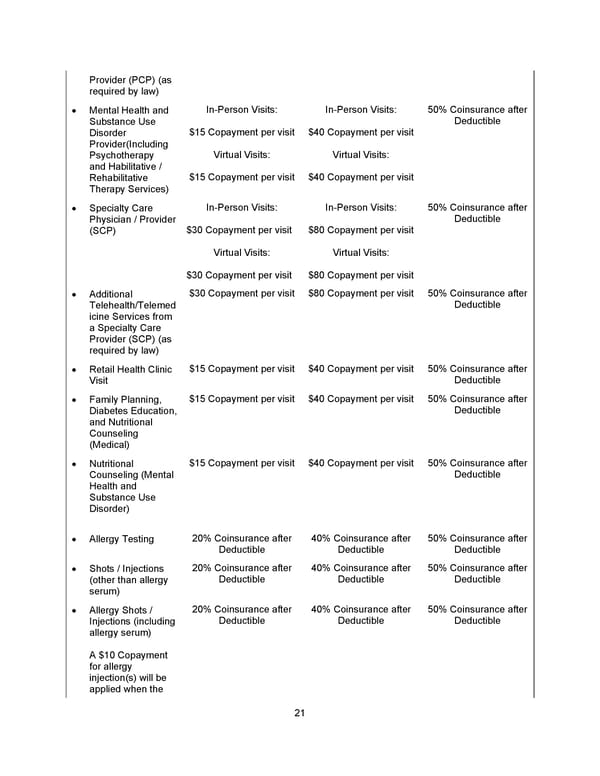
21 Provider (PCP) (as required by law) • Mental Health and Substance Use Disorder Provider ( Including Psychotherapy and Habilitative / Rehabilitative Therapy Services ) In - Person Visits: $15 Copayment per visit Virtual Visits: $15 Copayment per visit In - Person Visits: $40 Copayment per visit Virtual Visits: $40 Copayment per visit 50% Coinsurance after Deductible • Specialty Care Physician / Provider (SCP) In - Person Visits: $30 Copayment per visit Virtual Visits: $30 Copayment per visit In - Person Visits: $80 Copayment per visit Virtual Visits: $80 Copayment per visit 50% Coinsurance after Deductible • Additional Telehealth/Telemed icine Services from a Specialty Care Provider (SCP) (as required by law) $30 Copayment per visit $80 Copayment per visit 50% Coinsurance after Deductible • Retail Health Clinic Visit $15 Copayment per visit $40 Copayment per visit 50% Coinsurance after Deductible • Family Planning, Diabetes Education, and Nutritional Counseling (Medical) $15 Copayment per visit $40 Copayment per visit 50% Coinsurance after Deductible • Nutritional Counseling (Mental Health and Substance Use Disorder) $15 Copayment per visit $40 Copayment per visit 50% Coinsurance after Deductible • Allergy Testing 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Shots / Injections (other than allergy serum) 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Allergy Shots / Injections (including allergy serum) A $10 Copayment for allergy injection(s) will be applied when the 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible
 Benefit Booklet: Plan 1 Page 21 Page 23
Benefit Booklet: Plan 1 Page 21 Page 23