
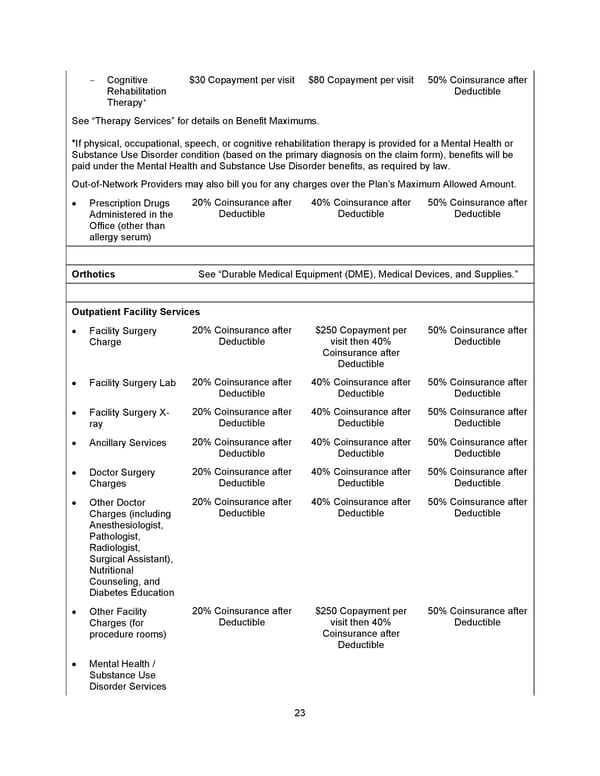
23 - Cognitive Rehabilitation Therapy + $30 Copayment per visit $80 Copayment per visit 50% Coinsurance after Deductible See “Therapy Services” for details on Benefit Maximums. + If physical , occupational , speech , or cognitive rehabilitation therapy is provided for a Mental Health or Substance Use Disorder condition (based on the primary diagnosis on the claim form) , benefits will be paid under the Mental Health and Substance Use Disorder benefits, as required by law . Out - of - Network Providers may also bill you for any charges over the Plan’s Maximum Allowed Amount. • Prescription Drugs Administered in the Office (other than allergy serum) 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible Orthotics See “ Durable Medical Equipment (DME), Medical Devices, and Supplies. ” Outpatient Facility Services • Facility Surgery Charge 20% Coinsurance after Deductible $250 Copayment per visit then 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Facility Surgery Lab 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Facility Surgery X - ray 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Ancillary Services 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Doctor Surgery Charges 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Other Doctor Charges (including Anesthesiologist, Pathologist, Radiologist, Surgical Assistant), Nutritional Counseling, and Diabetes Education 20% Coinsurance after Deductible 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Other Facility Charges (for procedure rooms) 20% Coinsurance after Deductible $250 Copayment per visit then 40% Coinsurance after Deductible 50% Coinsurance after Deductible • Mental Health / Substance Use Disorder Services
 Benefit Booklet: Plan 1 Page 23 Page 25
Benefit Booklet: Plan 1 Page 23 Page 25