
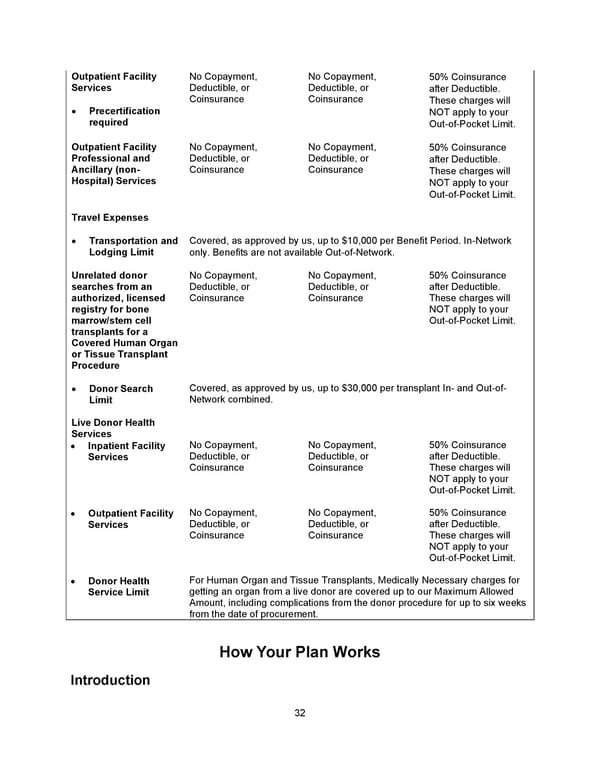
32 Outpatient Facility Services • Precertification required No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance 50% Coinsurance after Deductible. These charges will NOT apply to your Out-of-Pocket Limit. Outpatient Facility Professional and Ancillary (non- Hospital) Services No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance 50% Coinsurance after Deductible. These charges will NOT apply to your Out-of-Pocket Limit. Travel Expenses • Transportation and Lodging Limit Covered, as approved by us, up to $10,000 per Benefit Period. In-Network only. Benefits are not available Out-of-Network. Unrelated donor searches from an authorized, licensed registry for bone marrow/stem cell transplants for a Covered Human Organ or Tissue Transplant Procedure No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance 50% Coinsurance after Deductible. These charges will NOT apply to your Out-of-Pocket Limit. • Donor Search Limit Covered, as approved by us, up to $30,000 per transplant In- and Out-of- Network combined. Live Donor Health Services • Inpatient Facility Services No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance 50% Coinsurance after Deductible. These charges will NOT apply to your Out-of-Pocket Limit. • Outpatient Facility Services No Copayment, Deductible, or Coinsurance No Copayment, Deductible, or Coinsurance 50% Coinsurance after Deductible. These charges will NOT apply to your Out-of-Pocket Limit. • Donor Health Service Limit For Human Organ and Tissue Transplants, Medically Necessary charges for getting an organ from a live donor are covered up to our Maximum Allowed Amount, including complications from the donor procedure for up to six weeks from the date of procurement. How Your Plan Works Introduction
 Benefit Booklet: Plan 2 Page 32 Page 34
Benefit Booklet: Plan 2 Page 32 Page 34