
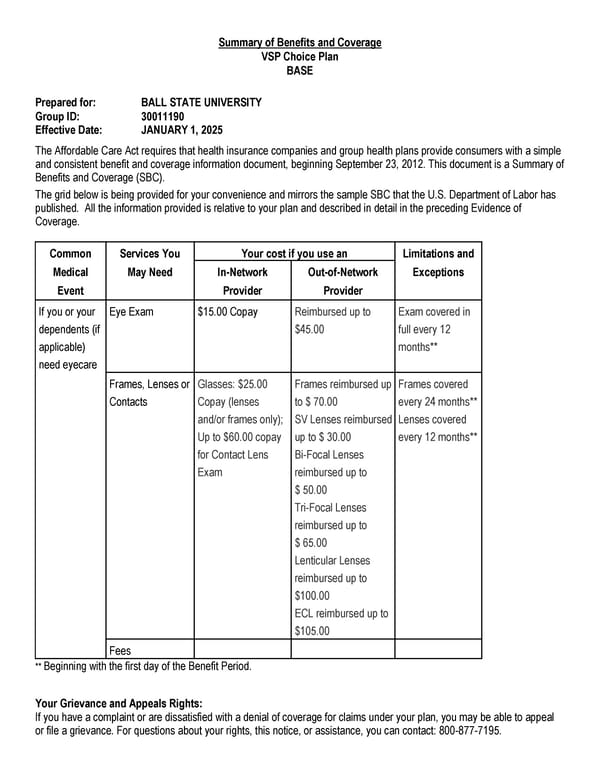
Summary of Benefits and Coverage VSP Choice Plan BASE Prepared for: BALL STATE UNIVERSITY Group ID: 30011190 Effective Date: JANUARY 1, 2025 The Affordable Care Act requires that health insurance companies and group health plans provide consumers with a simple and consistent benefit and coverage information document, beginning September 23, 2012. This document is a Summary of Benefits and Coverage (SBC). The grid below is being provided for your convenience and mirrors the sample SBC that the U.S. Department of Labor has published. All the information provided is relative to your plan and described in detail in the preceding Evidence of Coverage. Common Services You Your cost if you use an Limitations and Medical May Need In-Network Out-of-Network Exceptions Event Provider Provider If you or your dependents (if applicable) need eyecare Eye Exam $15.00 Copay Reimbursed up to $45.00 Exam covered in full every 12 months** Frames, Lenses or Contacts Glasses: $25.00 Copay (lenses and/or frames only); Up to $60.00 copay for Contact Lens Exam Frames reimbursed up to $ 70.00 SV Lenses reimbursed up to $ 30.00 Bi-Focal Lenses reimbursed up to $ 50.00 Tri-Focal Lenses reimbursed up to $ 65.00 Lenticular Lenses reimbursed up to $100.00 ECL reimbursed up to $105.00 Frames covered every 24 months** Lenses covered every 12 months** Fees ** Beginning with the first day of the Benefit Period. Your Grievance and Appeals Rights: If you have a complaint or are dissatisfied with a denial of coverage for claims under your plan, you may be able to appeal or file a grievance. For questions about your rights, this notice, or assistance, you can contact: 800-877-7195.
 Certificate of Coverage Page 22
Certificate of Coverage Page 22