
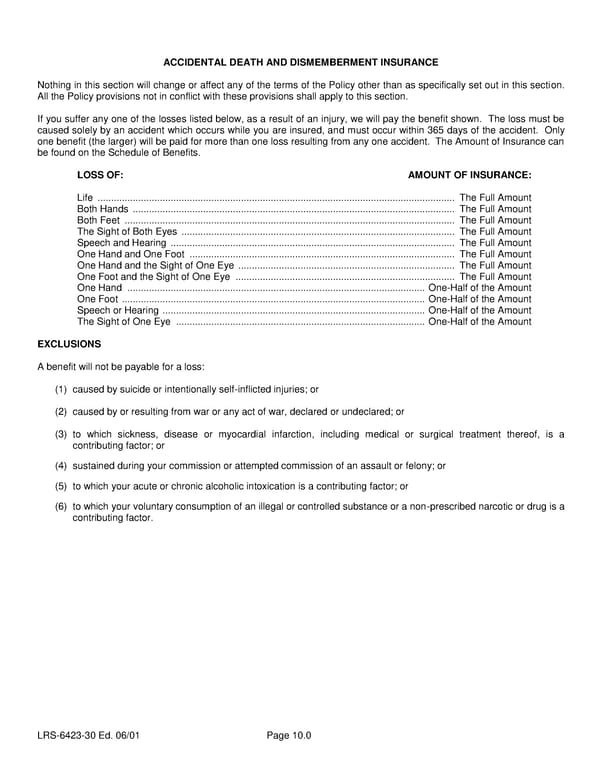
ACCIDENTAL DEATH AND DISMEMBERMENT INSURANCE Nothing in this section will change or affect any of the terms of the Policy other than as specifically set out in this section. All the Policy provisions not in conflict with these provisions shall apply to this section. If you suffer any one of the losses listed below, as a result of an injury, we will pay the benefit shown. The loss must be caused solely by an accident which occurs while you are insured, and must occur within 365 days of the accident. Only one benefit (the larger) will be paid for more than one loss resulting from any one accident. The Amount of Insurance can be found on the Schedule of Benefits. LOSS OF: AMOUNT OF INSURANCE: Life .................................................................................................................................... The Full Amount Both Hands ....................................................................................................................... The Full Amount Both Feet .......................................................................................................................... The Full Amount The Sight of Both Eyes ..................................................................................................... The Full Amount Speech and Hearing ......................................................................................................... The Full Amount One Hand and One Foot .................................................................................................. The Full Amount One Hand and the Sight of One Eye ................................................................................ The Full Amount One Foot and the Sight of One Eye ................................................................................. The Full Amount One Hand .............................................................................................................. One-Half of the Amount One Foot ................................................................................................................ One-Half of the Amount Speech or Hearing ................................................................................................. One-Half of the Amount The Sight of One Eye ............................................................................................ One-Half of the Amount EXCLUSIONS A benefit will not be payable for a loss: (1) caused by suicide or intentionally self-inflicted injuries; or (2) caused by or resulting from war or any act of war, declared or undeclared; or (3) to which sickness, disease or myocardial infarction, including medical or surgical treatment thereof, is a contributing factor; or (4) sustained during your commission or attempted commission of an assault or felony; or (5) to which your acute or chronic alcoholic intoxication is a contributing factor; or (6) to which your voluntary consumption of an illegal or controlled substance or a non-prescribed narcotic or drug is a contributing factor. LRS-6423-30 Ed. 06/01 Page 10.0
 Class 1 Group Life (Basic and Term) Certificate Page 12 Page 14
Class 1 Group Life (Basic and Term) Certificate Page 12 Page 14