
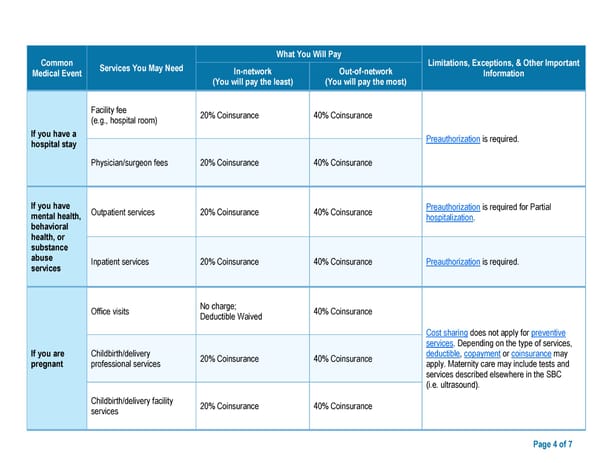
Common What You Will Pay Limitations, Exceptions, & Other Important Medical Event Services You May Need In-network Out-of-network Information (You will pay the least) (You will pay the most) Facility fee 20% Coinsurance 40% Coinsurance (e.g., hospital room) If you have a Preauthorization is required. hospital stay Physician/surgeon fees 20% Coinsurance 40% Coinsurance If you have Outpatient services 20% Coinsurance 40% Coinsurance Preauthorization is required for Partial mental health, hospitalization. behavioral health, or substance abuse Inpatient services 20% Coinsurance 40% Coinsurance Preauthorization is required. services Office visits No charge; 40% Coinsurance Deductible Waived Cost sharing does not apply for preventive services. Depending on the type of services, If you are Childbirth/delivery 20% Coinsurance 40% Coinsurance deductible, copayment or coinsurance may pregnant professional services apply. Maternity care may include tests and services described elsewhere in the SBC (i.e. ultrasound). Childbirth/delivery facility 20% Coinsurance 40% Coinsurance services Page 4 of 7
 ****Class Only Model Document *** Page 3 Page 5
****Class Only Model Document *** Page 3 Page 5