
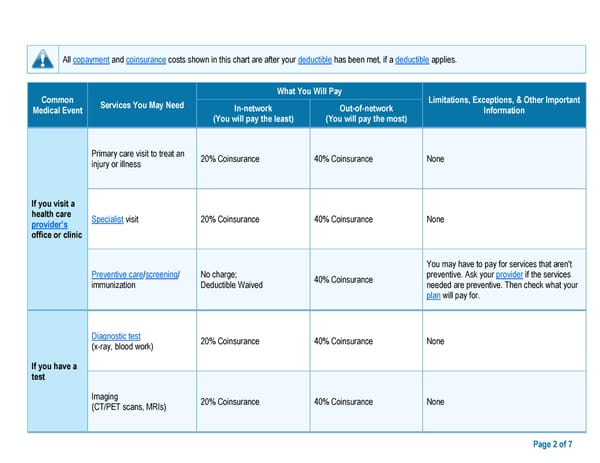
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies. Common What You Will Pay Limitations, Exceptions, & Other Important Medical Event Services You May Need In-network Out-of-network Information (You will pay the least) (You will pay the most) Primary care visit to treat an 20% Coinsurance 40% Coinsurance None injury or illness If you visit a health care Specialist visit 20% Coinsurance 40% Coinsurance None provider’s office or clinic You may have to pay for services that aren't Preventive care/screening/ No charge; 40% Coinsurance preventive. Ask your provider if the services immunization Deductible Waived needed are preventive. Then check what your plan will pay for. Diagnostic test 20% Coinsurance 40% Coinsurance None (x-ray, blood work) If you have a test Imaging 20% Coinsurance 40% Coinsurance None (CT/PET scans, MRIs) Page 2 of 7
 ****Class Only Model Document *** Page 1 Page 3
****Class Only Model Document *** Page 1 Page 3