
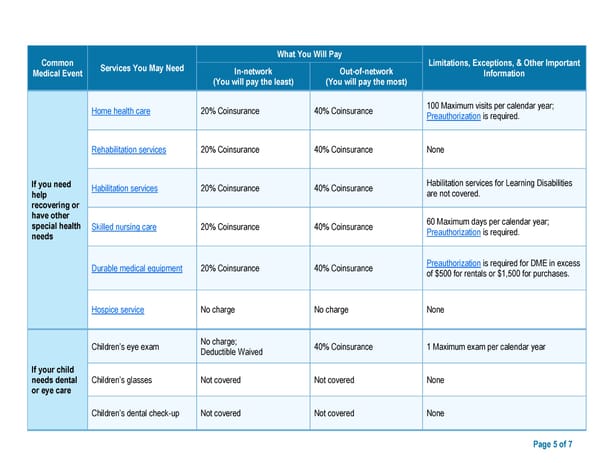
Common What You Will Pay Limitations, Exceptions, & Other Important Medical Event Services You May Need In-network Out-of-network Information (You will pay the least) (You will pay the most) Home health care 20% Coinsurance 40% Coinsurance 100 Maximum visits per calendar year; Preauthorization is required. Rehabilitation services 20% Coinsurance 40% Coinsurance None If you need Habilitation services 20% Coinsurance 40% Coinsurance Habilitation services for Learning Disabilities help are not covered. recovering or have other 60 Maximum days per calendar year; special health Skilled nursing care 20% Coinsurance 40% Coinsurance Preauthorization is required. needs Durable medical equipment 20% Coinsurance 40% Coinsurance Preauthorization is required for DME in excess of $500 for rentals or $1,500 for purchases. Hospice service No charge No charge None Children’s eye exam No charge; 40% Coinsurance 1 Maximum exam per calendar year Deductible Waived If your child needs dental Children’s glasses Not covered Not covered None or eye care Children’s dental check-up Not covered Not covered None Page 5 of 7
 ****Class Only Model Document *** Page 4 Page 6
****Class Only Model Document *** Page 4 Page 6