
Dental Insurance Plan Summary
This document provides a summary of dental insurance coverage and benefits including in-network and out-of-network services, deductibles, annual maximum benefits, and a list of primary covered services and limitations.
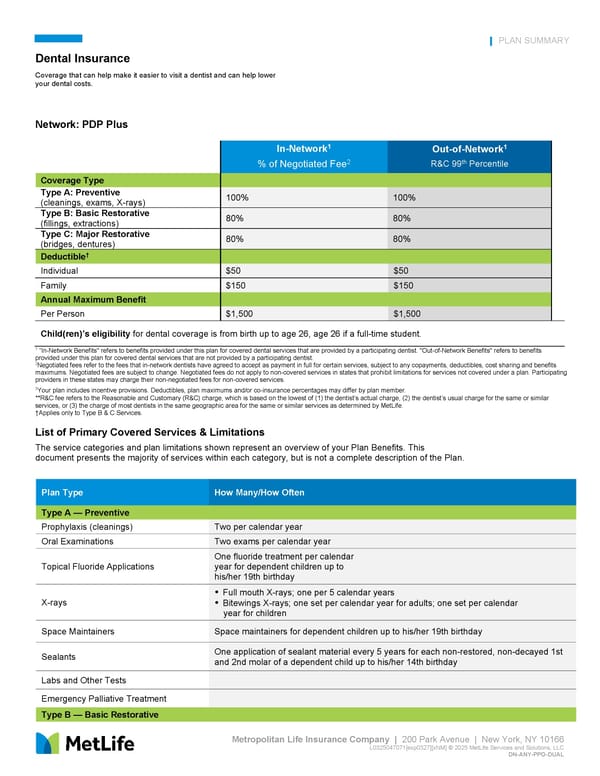
Metropolitan Life Insurance Company | 200 Park Avenue | New York, NY 10166 L0325047071[exp0327][xNM] © 2025 MetLife Services and Solutions, LLC DN-ANY-PPO-DUAL PLAN SUMMARY Dental Insurance Coverage that can help make it easier to visit a dentist and can help lower your dental costs. Network: PDP Plus Deductible† Individual $50 $50 Family $150 $150 Annual Maximum Benefit Per Person $1,500 $1,500 Child(ren)’s eligibility for dental coverage is from birth up to age 26, age 26 if a full-time student. 1 “In-Network Benefits" refers to benefits provided under this plan for covered dental services that are provided by a participating dentist. "Out-of-Network Benefits" refers to benefits provided under this plan for covered dental services that are not provided by a participating dentist. 2Negotiated fees refer to the fees that in-network dentists have agreed to accept as payment in full for certain services, subject to any copayments, deductibles, cost sharing and benefits maximums. Negotiated fees are subject to change. Negotiated fees do not apply to non-covered services in states that prohibit limitations for services not covered under a plan. Participating providers in these states may charge their non-negotiated fees for non-covered services. 3Your plan includes incentive provisions. Deductibles, plan maximums and/or co-insurance percentages may differ by plan member. **R&C fee refers to the Reasonable and Customary (R&C) charge, which is based on the lowest of (1) the dentist’s actual charge, (2) the dentist’s usual charge for the same or similar services, or (3) the charge of most dentists in the same geographic area for the same or similar services as determined by MetLife. †Applies only to Type B & C Services. List of Primary Covered Services & Limitations The service categories and plan limitations shown represent an overview of your Plan Benefits. This document presents the majority of services within each category, but is not a complete description of the Plan. In-Network1 % of Negotiated Fee2 Out-of-Network1 R&C 99th Percentile Coverage Type Type A: Preventive (cleanings, exams, X-rays) 100% 100% Type B: Basic Restorative (fillings, extractions) 80% 80% Type C: Major Restorative (bridges, dentures) 80% 80% Plan Type How Many/How Often Type A — Preventive Prophylaxis (cleanings) Two per calendar year Oral Examinations Two exams per calendar year Topical Fluoride Applications One fluoride treatment per calendar year for dependent children up to his/her 19th birthday X-rays Full mouth X-rays; one per 5 calendar years Bitewings X-rays; one set per calendar year for adults; one set per calendar year for children Space Maintainers Space maintainers for dependent children up to his/her 19th birthday Sealants One application of sealant material every 5 years for each non-restored, non-decayed 1st and 2nd molar of a dependent child up to his/her 14th birthday Labs and Other Tests Emergency Palliative Treatment Type B — Basic Restorative
 Dental Insurance Plan Summary Page 2
Dental Insurance Plan Summary Page 2