
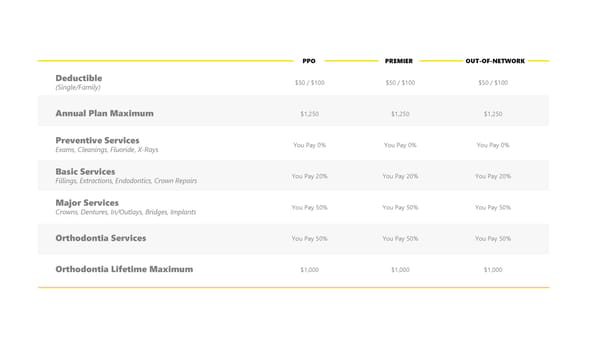
PPO PREMIER OUT-OF-NETWORK Deductible $50 / $100 $50 / $100 $50 / $100 (Single/Family) Annual Plan Maximum $1,250 $1,250 $1,250 Preventive Services You Pay 0% You Pay 0% You Pay 0% Exams, Cleanings, Fluoride, X-Rays Basic Services You Pay 20% You Pay 20% You Pay 20% Fillings, Extractions, Endodontics, Crown Repairs Major Services You Pay 50% You Pay 50% You Pay 50% Crowns, Dentures, In/Outlays, Bridges, Implants Orthodontia Services You Pay 50% You Pay 50% You Pay 50% Orthodontia Lifetime Maximum $1,000 $1,000 $1,000
 DePauw University 2025 Benefit Guide Page 21 Page 23
DePauw University 2025 Benefit Guide Page 21 Page 23