DePauw University 2026 Post 65 Retiree Benefits Package
An overview of the retiree medical program and benefits available to current enrollees at DePauw University, with a deadline for changes set to December 5th, 2025.
Retiree Medical Program • AmWins Group Benefits 2026 Post-65 Retiree Benefits Current Enrollees Must Make Changes By: December 5th, 2025
Medical & Rx Monthly Payment Summary | Hire Date Before 7/1/2005 Dental Monthly Rate Retiree $22.12 Retiree + Spouse $63.40 Vision Monthly Rate Retiree $8.38 Retiree + Spouse $13.19 Retiree + Child(ren) $14.15 Retiree + Family $20.55 Rx Low Plan 1 Rx Mid Plan 2 Rx High Plan 3 Per Person Covered $123.99 $187.00 $299.17 How to pay? Mail a check for your first month’s premium to: DePauw University/AmWins Group Benefits, Inc. 50 Whitecap Drive, North Kingstown, RI 02852
Medical & Rx Monthly Payment Summary | Hire Date Between 7/1/2005 – 1/1/2013 Dental Monthly Rate Retiree $32.86 Retiree + Spouse $81.94 Vision Rx Low Plan 1 Rx Mid Plan 2 Rx High Plan 3 Per Person Covered $315.30 $349.80 $376.60 How to pay? Mail a check for your first month’s premium to: DePauw University/AmWins Group Benefits, Inc. 50 Whitecap Drive, North Kingstown, RI 02852 Monthly Rate Retiree $8.38 Retiree + Spouse $13.19 Retiree + Child(ren) $14.15 Retiree + Family $20.55
Services Medicare Pays Plan Pays You Pay HOSPITAL CONFINEMENT BENEFIT* Semiprivate room and board, general nursing and miscellaneous services and supplies: First 60 days All but Part A Deductible Part A Deductible $0 61st through 90th day All but Part A Coinsurance Part A Coinsurance $0 91st through 150th day (While using 60 lifetime reserve days) All but Part A Coinsurance Part A Coinsurance $0 Once Lifetime Reserve days are used: Additional 365 days: Beyond the Additional 365 days $0 $0 100% of Medicare Eligible Expenses $0 $0 All costs SKILLED NURSING FACILITY CARE* You must meet Medicare's requirements, including having been in a hospital for at least 3 days and entered a Medicare-approved facility within 30 days after leaving the hospital: First 20 days All approved amounts $0 $0 21st through 100 th day All but Part A Coinsurance Part A Coinsurance $0 101 st day and after $0 $0 All costs BLOOD DEDUCTIBLE – Hospital Confinement and Out-Patient Medical Expense When furnished by a hospital or skilled nursing facility during a covered stay. First 3 pints $0 3 pints $0 Additional amounts 100% $0 $0 HOSPICE CARE Available as long as your doctor certifies you are terminally ill and you elect to receive these services. All but very limited coinsurance for outpatient drugs and inpatient respite care $0 Balance Medicare Hospital Services (Part A)
Medicare Medical Services (Part B) Services Medicare Pays Plan Pays You Pay OUT-PATIENT MEDICAL EXPENSES - In or Out of the Hospital and Out-Patient Hospital Treatment, such as Physician's services, inpatient and outpatient medical and surgical services and supplies, physical and speech therapy, diagnostic tests, durable medical equipment: Medicare Part B Deductible: First Medicare-approved amounts** $0 $0 Part B Deductible Next Medicare-approved amounts Generally 80% $0 20% until Calendar year deductible is met ($400) Next Medicare-approved amounts Generally 80% 16% 4% until Out Of Pocket Maximum is met ($1,250) Remainder of Medicare-approved amounts Generally 80% Generally 20% 0% Part B Excess Charges (Above Medicare Approve Amounts) $0 100% 0% BLOOD First 3 pints $0 All costs $0 Next Medicare Approved Amounts** $0 $0 Part B Deductible Next Medicare-approved amounts Generally 80% $0 20% until Calendar year deductible is met ($400) Next Medicare-approved amounts Generally 80% 16% 4% until Out Of Pocket Maximum is met ($1,250) Remainder of Medicare Approved Amounts 80% 20% $0 CLINICAL LABORATORY SERVICES Blood tests for Diagnostic Services 100% $0 $0
Services Medicare Pays Plan Pays You Pay HOME HEALTH CARE – Medicare Approved Services: Medically necessary skilled care services and medical supplies 100% $0 $0 DURABLE MEDICAL EQUIPMENT First of Medicare Approved Amounts** $0 $0 Part B Deductible Next Medicare-approved amounts Generally 80% $0 20% until Calendar year deductible is met ($400) Next Medicare-approved amounts Generally 80% 16% 4% until Out Of Pocket Maximum is met ($1,250) Remainder of Medicare Approved Amounts 80% 20% $0 Medicare Parts A & B Services Medicare Pays Plan Pays You Pay FOREIGN TRAVEL - Medically necessary emergency care services beginning during the first 60 days of each trip outside the USA: First $250 each calendar year $0 $0 $250 Remainder of charges $0 80% to a lifetime maximum of $50,000 20% and amounts over the $50,000 lifetime max Benefits Not Covered By Medicare
Rx COVERAGE Your plan uses a formulary – a list of covered drugs. The amount you pay depends on the drug’s tier and on the coverage stage that you’ve reached. From time to time, a drug may move to a different tier. If a drug you are taking is going to move to a higher (or more expensive) tier, or if the change limits your ability to fill a prescription, Express Scripts will notify you before the change is made. Express Scripts Website
Long-Term Care Pharmacy If you reside in an LTC facility, you pay the same as at a network retail pharmacy. LTC pharmacies must dispense brand-name drugs in amounts of 14 days or less at a time. They may also dispense less than a one month’s supply of generic drugs at a time. Contact your plan if you have questions about cost-sharing or billing when less than a one- month supply is dispensed. You must use Express Scripts Medicare network pharmacies to fill your prescriptions. Covered Medicare Part D drugs are available at out-of- network pharmacies only in special circumstances, such as illness while traveling outside of the plan’s service area where there is no network pharmacy. You generally have to pay the full cost for drugs received at an out-of-network pharmacy at the time you fill your prescription. You can ask us to reimburse you for our share of the cost. Please contact the plan or the Retiree Customer Service Center for more details. Out-of-Network Coverage Express Scripts Website See your prescription’s formulary tier on the Express Scripts website.
Rx Plan Option #1 Deductible Stage $615.00 Initial Coverage Stage After you pay your yearly deductible: You will pay the following until your total yearly drug costs (what you and the plan pay) reach $2,000 : Tier Retail One- Month (31-day) Supply Retail 3-Month (90-day) Supply (Standard) Home Delivery Three-Month (90- day) Supply Tier 1: Generic Drugs 15% 15% 10% Tier 2: Preferred Brand Drugs 30% 30% 25% Tier 3: Non- Preferred Brand 30% 30% 30% Tier 4: Specialty 25% 25% 25% If your doctor prescribes less than a full month’s supply of certain drugs, you will pay a daily cost-sharing rate based on the actual number of days of the drug that you receive. You may receive up to a 90-day supply of certain maintenance drugs (medications taken on a long-term basis) by mail through the Express Scripts PharmacySM. There is no charge for standard shipping. Not all drugs are available at a 90-day supply, and not all retail pharmacies offer a 90-day supply. Non-part D Drugs Covered; Excluding lifestyle Compound Compound Management Solution applies. Compound Management Solution is in place to mitigate compound drug abuse by means of inclusion and exclusion lists Catastrophic Coverage Stage After your yearly out-of-pocket drug costs reach $2,100, you will pay $0
Rx Plan Option #2 Deductible Stage $100.00 Initial Coverage Stage After you pay your yearly deductible: You will pay the following until your total yearly drug costs (what you and the plan pay) reach $2,000 : Tier Retail One- Month (31-day) Supply Retail 3-Month (90-day) Supply (Standard) Home Delivery Three-Month (90- day) Supply Tier 1: Generic Drugs 15% 15% 10% Tier 2: Preferred Brand Drugs 30% 30% 25% Tier 3: Non- Preferred Brand 50% 50% 50% Tier 4: Specialty 25% 25% 25% If your doctor prescribes less than a full month’s supply of certain drugs, you will pay a daily cost-sharing rate based on the actual number of days of the drug that you receive. You may receive up to a 90-day supply of certain maintenance drugs (medications taken on a long-term basis) by mail through the Express Scripts PharmacySM. There is no charge for standard shipping. Not all drugs are available at a 90-day supply, and not all retail pharmacies offer a 90-day supply. Non-part D Drugs Covered; Excluding lifestyle Compound Compound Management Solution applies. Compound Management Solution is in place to mitigate compound drug abuse by means of inclusion and exclusion lists Catastrophic Coverage Stage After your yearly out-of-pocket drug costs reach $2,100, you will pay $0
Rx Plan Option #3 Deductible Stage $100.00 Initial Coverage Stage After you pay your yearly deductible: You will pay the following until your total yearly drug costs (what you and the plan pay) reach $2,000 : Tier Retail One- Month (31-day) Supply Retail 3-Month (90-day) Supply (Standard) Home Delivery Three-Month (90- day) Supply Tier 1: Generic Drugs 15% 15% 10% Tier 2: Preferred Brand Drugs 30% 30% 25% Tier 3: Non- Preferred Brand 40% 40% 35% Tier 4: Specialty 25% 25% 25% If your doctor prescribes less than a full month’s supply of certain drugs, you will pay a daily cost-sharing rate based on the actual number of days of the drug that you receive. You may receive up to a 90-day supply of certain maintenance drugs (medications taken on a long-term basis) by mail through the Express Scripts PharmacySM. There is no charge for standard shipping. Not all drugs are available at a 90-day supply, and not all retail pharmacies offer a 90-day supply. Non-part D Drugs Covered; Excluding lifestyle Compound Compound Management Solution applies. Compound Management Solution is in place to mitigate compound drug abuse by means of inclusion and exclusion lists Catastrophic Coverage Stage After your yearly out-of-pocket drug costs reach $2,100, you will pay $0
DENTAL Delta Dental offers three levels of benefits coverage: PPO Dentist, Premier Dentist, and Non-Participating Dentist. Find providers, view your ID card, and more on the Delta Dental online portal or on their mobile app. Dental Coverage with Delta Dental DELTA DENTAL OF INDIANA 225 S East St Indianapolis, IN 46202 317-842-4022 KRISTEN JONES Group Delta Dental PPO Online Portal Download the App
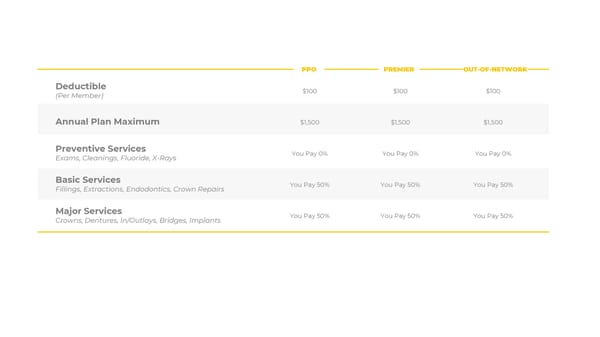
Deductible (Per Member) $100 $100 $100 Annual Plan Maximum $1,500 $1,500 $1,500 Preventive Services Exams, Cleanings, Fluoride, X-Rays You Pay 0% You Pay 0% You Pay 0% Basic Services Fillings, Extractions, Endodontics, Crown Repairs You Pay 50% You Pay 50% You Pay 50% Major Services Crowns, Dentures, In/Outlays, Bridges, Implants You Pay 50% You Pay 50% You Pay 50% OUT-OF-NETWORK PPO PREMIER
VISION Anthem Blue Cross and Blue Shield vision members have access to one of the nation’s largest network of vision providers. Blue View Vision is the only network that gives you the ability to use in-network benefits at 1-800- CONTACTS, or choose a private eye doctor, or go to retail vendors. Vision Coverage through Anthem Online Portal
Routine eye exams, glasses lenses, and contacts available once every 12 months. Frames available once every 24 months. Exam $10 copay $42 allowance Glasses Lenses (Single / Bifocal/ Trifocal) $10 copay $40 - $80 allowance Glasses Frames $130 retail frame allowance + 20% off remaining balance $45 allowance Contact Lenses (Medically Necessary / Elective) Covered in Full / $130 allowance $210 allowance / $105 allowance In-Network Out-of-Network
TIAA • TIAA Login • How to update your TIAA beneficiary information HUB HUB provides participant education via in- person or virtual meetings, as often as needed. This improves participant access to high quality retirement planning. Multi-Employer Retirement Plan (MEP) | 403(b) Schedule a Financial Planning Session Retirement Health Care Savings (VEBA) for employees hired before 2013. Eligible retirees with a balance may be reimbursed for qualifying medical expenses by using funds from their Retirement Health Care Savings (VEBA). Learn more. VEBA
If you are suffering from a mental health condition, have hope: you are not alone. Depression, anxiety, substance use disorders, trauma, and other conditions affect people from all walks of life. Below are just a few resources available. Mental Health BENEFITS Support & Resources BeWell Indiana In addition to mental health resources, there are a wide range of free resources for Hoosiers available here. For example, help with substance use disorder & recovery resources, child care solutions, and more. You can start by calling 2-1-1. For crisis help text the word “HOME” to 741741.
How to Enroll • Review the information on this website. • Complete and sign the enrollment form. • Return your enrolment form and the first month’s premium in a postage-paid return envelope. Get Enrolled Today! Enrollment Form If you have any questions, contact the AmWins Group Benefits Customer Care Center toll-free 1-888-883-3757 Monday – Friday, 8AM – 8PM EST
Frequently Asked Questions 1. Who can I call if I have questions? 2. How does the plan work? 3. Can my age 65 spouse enroll if I am not yet age 65? 4. My spouse is not yet 65. What will happen to coverage for my spouse after I enroll in the plan? 5. Will I have to re-enroll in the Plan next year? 6. When will I receive my ID cards? 7. How are my medical claims paid? 8. Do I still need my Medicare ID Card? 9. Do my prescription drug co-payments count toward my medical plan deductible? 10. How do I get my prescriptions filled? 11. Where can I get information on using Mail Order Services? Hover over the ! Icon by each question to see the answer.
12. How can I find out if my drugs are covered on the new plan? 13. How can I lower my drug expenses? 14. What services are not covered? 15. If I choose not to enroll this year can I enroll next year? 16. Do I have the option to enroll in just medical or Rx coverage, or do I have to do both? 17. How do I pay for my coverage? 18. Can I enroll in a separate Medicare Part D plan and the AmWins medical Rx plan? 19. How do I obtain a replacement ID card for my plans? 20. What happens to coverage for a spouse if the retiree dies?