
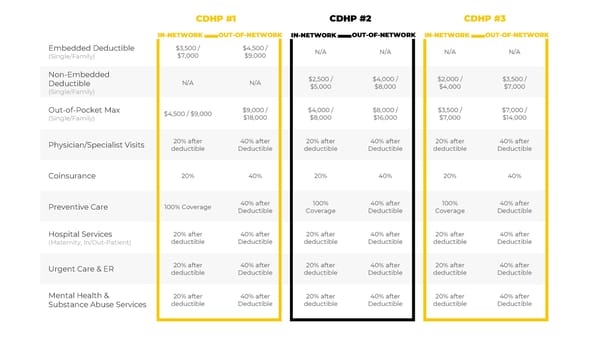
Embedded Deductible (Single/Family) $3,500 / $7,000 $4,500 / $9,000 N/A N/A N/A N/A Non-Embedded Deductible (Single/Family) N/A N/A $2,500 / $5,000 $4,000 / $8,000 $2,000 / $4,000 $3,500 / $7,000 Out-of-Pocket Max (Single/Family) $4,500 / $9,000 $9,000 / $18,000 $4,000 / $8,000 $8,000 / $16,000 $3,500 / $7,000 $7,000 / $14,000 Physician/Specialist Visits 20% after deductible 40% after Deductible 20% after deductible 40% after Deductible 20% after deductible 40% after Deductible Coinsurance 20% 40% 20% 40% 20% 40% Preventive Care 100% Coverage 40% after Deductible 100% Coverage 40% after Deductible 100% Coverage 40% after Deductible Hospital Services (Maternity, In/Out-Patient) 20% after deductible 40% after Deductible 20% after deductible 40% after Deductible 20% after deductible 40% after Deductible Urgent Care & ER 20% after deductible 40% after Deductible 20% after deductible 40% after Deductible 20% after deductible 40% after Deductible Mental Health & Substance Abuse Services 20% after deductible 40% after Deductible 20% after deductible 40% after Deductible 20% after deductible 40% after Deductible CDHP #1 CDHP #2 CDHP #3 OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK IN-NETWORK
 DePauw University: Your Employee Benefits Package Page 9 Page 11
DePauw University: Your Employee Benefits Package Page 9 Page 11