
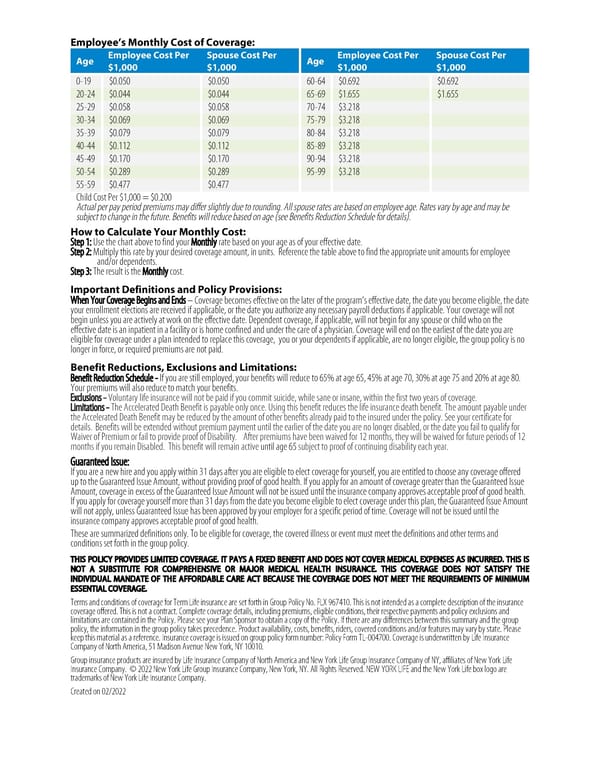
Employee’sMonthly Cost of Coverage: Age Employee Cost Per Spouse Cost Per Age Employee Cost Per Spouse Cost Per $1,000 $1,000 $1,000 $1,000 0-19 $0.050 $0.050 60-64 $0.692 $0.692 20-24 $0.044 $0.044 65-69 $1.655 $1.655 25-29 $0.058 $0.058 70-74 $3.218 30-34 $0.069 $0.069 75-79 $3.218 35-39 $0.079 $0.079 80-84 $3.218 40-44 $0.112 $0.112 85-89 $3.218 45-49 $0.170 $0.170 90-94 $3.218 50-54 $0.289 $0.289 95-99 $3.218 55-59 $0.477 $0.477 Child Cost Per $1,000 = $0.200 Actual per pay period premiums may differ slightly due to rounding. All spouse rates are based on employee age. Rates vary by age and may be subject to change in the future. Benefits will reduce based on age (see Benefits Reduction Schedule for details). How to Calculate YourMonthly Cost: Step 1: Use the chart above to find your Monthly rate based on your age as of your effective date. Step 2: Multiply this rate by your desired coverage amount, in units. Reference the table above to find the appropriate unit amounts for employee and/or dependents. Step 3: The result is the Monthly cost. Important Definitions and Policy Provisions: WhenYourCoverageBeginsandEnds–Coverage becomes effective on the later of the program’s effective date, the date you become eligible, the date your enrollment elections are received if applicable, or the date you authorize any necessary payroll deductions if applicable. Your coverage will not begin unless you are actively at work on the effective date. Dependent coverage, if applicable, will not begin for any spouse or child who on the effective date is an inpatient in a facility or is home confined and under the care of a physician. Coverage will end on the earliest of the date you are eligible for coverage under a plan intended to replace this coverage, you or your dependents if applicable, are no longer eligible, the group policy is no longer in force, or required premiums are not paid. Benefit Reductions, Exclusions and Limitations: Benefit Reduction Schedule - If you are still employed, your benefits will reduce to 65% at age 65, 45% at age 70, 30% at age 75 and 20% at age 80. Your premiums will also reduce to match your benefits. Exclusions - Voluntary life insurance will not be paid if you commit suicide, while sane or insane, within the first two years of coverage. Limitations - The Accelerated Death Benefit is payable only once. Using this benefit reduces the life insurance death benefit. The amount payable under the Accelerated Death Benefit may be reduced by the amount of other benefits already paid to the insured under the policy. See your certificate for details. Benefits will be extended without premium payment until the earlier of the date you are no longer disabled, or the date you fail to qualify for Waiver of Premium or fail to provide proof of Disability. After premiums have been waived for 12 months, they will be waived for future periods of 12 months if you remain Disabled. This benefit will remain active until age 65 subject to proof of continuing disability each year. Guaranteed Issue: If you are a new hire and you apply within 31 days after you are eligible to elect coverage for yourself, you are entitled to choose any coverage offered up to the Guaranteed Issue Amount, without providing proof of good health. If you apply for an amount of coverage greater than the Guaranteed Issue Amount, coverage in excess of the Guaranteed Issue Amount will not be issued until the insurance company approves acceptable proof of good health. If you apply for coverage yourself more than 31 days from the date you become eligible to elect coverage under this plan, the Guaranteed Issue Amount will not apply, unless Guaranteed Issue has been approved by your employer for a specific period of time. Coverage will not be issued until the insurance company approves acceptable proof of good health. These are summarized definitions only. To be eligible for coverage, the covered illness or event must meet the definitions and other terms and conditions set forth in the group policy. THIS POLICY PROVIDES LIMITED COVERAGE. IT PAYS A FIXED BENEFIT AND DOES NOT COVER MEDICAL EXPENSES AS INCURRED. THIS IS NOT A SUBSTITUTE FOR COMPREHENSIVE OR MAJOR MEDICAL HEALTH INSURANCE. THIS COVERAGE DOES NOT SATISFY THE INDIVIDUAL MANDATE OF THE AFFORDABLE CARE ACT BECAUSE THE COVERAGE DOES NOT MEET THE REQUIREMENTS OF MINIMUM ESSENTIAL COVERAGE. Terms and conditions of coverage for Term Life insurance are set forth in Group Policy No. FLX 967410. This is not intended as a complete description of the insurance coverage offered. This is not a contract. Complete coverage details, including premiums, eligible conditions, their respective payments and policy exclusions and limitations are contained in the Policy. Please see your Plan Sponsor to obtain a copy of the Policy. If there are any differences between this summary and the group policy, the information in the group policy takes precedence. Product availability, costs, benefits, riders, covered conditions and/or features may vary by state. Please keep this material as a reference. Insurance coverage is issued on group policy form number: Policy Form TL-004700. Coverage is underwritten by Life Insurance Company of North America, 51 Madison Avenue New York, NY 10010. Group insurance products are insured by Life Insurance Company of North America and New York Life Group Insurance Company of NY, affiliates of New York Life Insurance Company. ©2022New York Life Group Insurance Company, New York, NY. All Rights Reserved. NEW YORK LIFE and the New York Life box logo are trademarks of New York Life Insurance Company. Created on 02/2022
 Employee-Paid Term Life Insurance Page 1
Employee-Paid Term Life Insurance Page 1