
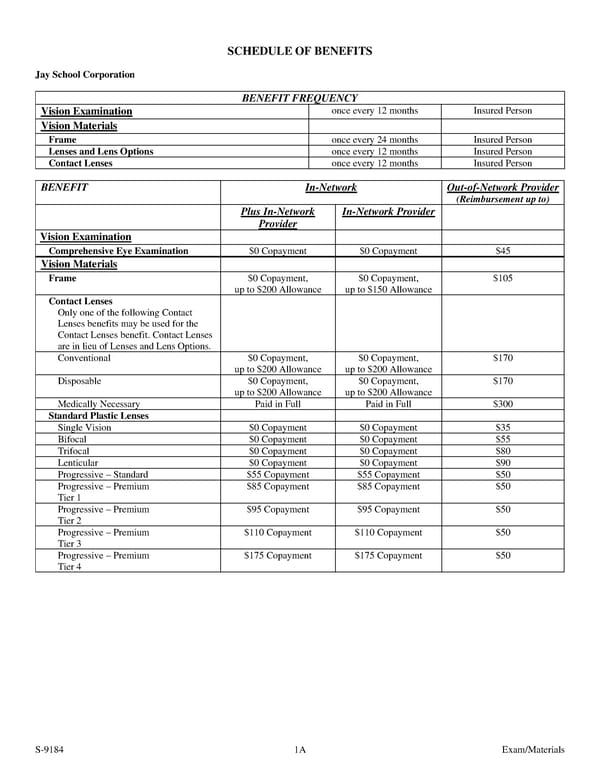
SCHEDULE OF BENEFITS Jay School Corporation BENEFIT FREQUENCY Vision Examination once every 12 months Insured Person Vision Materials Frame once every 24 months Insured Person Lenses and Lens Options once every 12 months Insured Person Contact Lenses once every 12 months Insured Person BENEFIT In-Network Out-of-Network Provider (Reimbursement up to) Plus In-Network In-Network Provider Provider Vision Examination Comprehensive Eye Examination $0 Copayment $0 Copayment $45 Vision Materials Frame $0 Copayment, $0 Copayment, $105 up to $200 Allowance up to $150 Allowance Contact Lenses Only one of the following Contact Lenses benefits may be used for the Contact Lenses benefit. Contact Lenses are in lieu of Lenses and Lens Options. Conventional $0 Copayment, $0 Copayment, $170 up to $200 Allowance up to $200 Allowance Disposable $0 Copayment, $0 Copayment, $170 up to $200 Allowance up to $200 Allowance Medically Necessary Paid in Full Paid in Full $300 Standard Plastic Lenses Single Vision $0 Copayment $0 Copayment $35 Bifocal $0 Copayment $0 Copayment $55 Trifocal $0 Copayment $0 Copayment $80 Lenticular $0 Copayment $0 Copayment $90 Progressive – Standard $55 Copayment $55 Copayment $50 Progressive – Premium $85 Copayment $85 Copayment $50 Tier 1 Progressive – Premium $95 Copayment $95 Copayment $50 Tier 2 Progressive – Premium $110 Copayment $110 Copayment $50 Tier 3 Progressive – Premium $175 Copayment $175 Copayment $50 Tier 4 S-9184 1A Exam/Materials
 Fidelity Security Life Insurance Company Group Vision Insurance Policy Page 11 Page 13
Fidelity Security Life Insurance Company Group Vision Insurance Policy Page 11 Page 13