
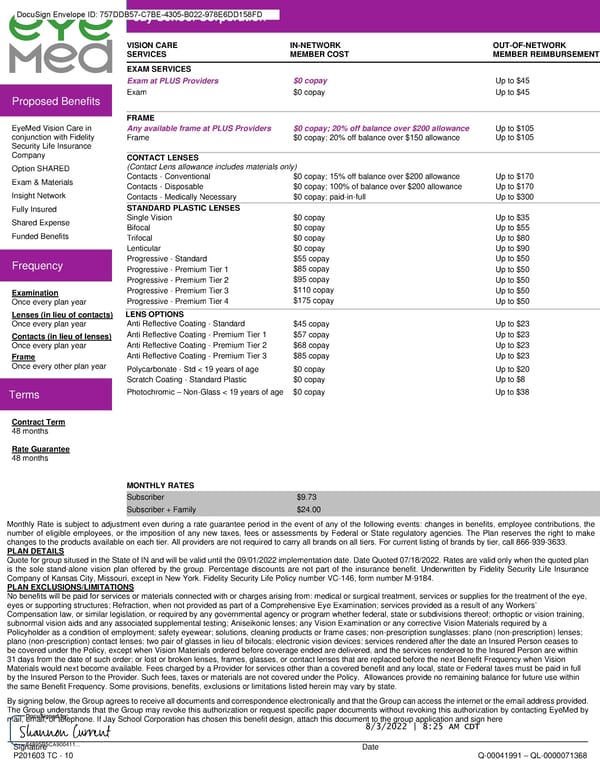
DocuSign Envelope ID: 757DDB57-C7BE-4305-B022-978E6DD158FD Jay School Corporation VISION CARE IN-NETWORK OUT-OF-NETWORK SERVICES MEMBER COST MEMBER REIMBURSEMENT EXAM SERVICES Exam at PLUS Providers $0 copay Up to $45 Exam $0 copay Up to $45 Proposed Benefits FRAME EyeMed Vision Care in Any available frame at PLUS Providers $0 copay; 20% off balance over $200 allowance Up to $105 conjunction with Fidelity Frame $0 copay; 20% off balance over $150 allowance Up to $105 Security Life Insurance Company CONTACT LENSES Option SHARED (Contact Lens allowance includes materials only) Exam & Materials Contacts - Conventional $0 copay; 15% off balance over $200 allowance Up to $170 Contacts - Disposable $0 copay; 100% of balance over $200 allowance Up to $170 Insight Network Contacts - Medically Necessary $0 copay; paid-in-full Up to $300 Fully Insured STANDARD PLASTIC LENSES Shared Expense Single Vision $0 copay Up to $35 Bifocal $0 copay Up to $55 Funded Benefits Trifocal $0 copay Up to $80 Lenticular $0 copay Up to $90 Frequency Progressive - Standard $55 copay Up to $50 Progressive - Premium Tier 1 $85 copay Up to $50 Progressive - Premium Tier 2 $95 copay Up to $50 Examination Progressive - Premium Tier 3 $110 copay Up to $50 Once every plan year Progressive - Premium Tier 4 $175 copay Up to $50 Lenses (in lieu of contacts) LENS OPTIONS Once every plan year Anti Reflective Coating - Standard $45 copay Up to $23 Contacts (in lieu of lenses) Anti Reflective Coating - Premium Tier 1 $57 copay Up to $23 Once every plan year Anti Reflective Coating - Premium Tier 2 $68 copay Up to $23 Frame Anti Reflective Coating - Premium Tier 3 $85 copay Up to $23 Once every other plan year Polycarbonate - Std < 19 years of age $0 copay Up to $20 Scratch Coating - Standard Plastic $0 copay Up to $8 Terms Photochromic – Non-Glass < 19 years of age $0 copay Up to $38 Contract Term 48 months Rate Guarantee 48 months MONTHLY RATES Subscriber $9.73 Subscriber + Family $24.00 Monthly Rate is subject to adjustment even during a rate guarantee period in the event of any of the following events: changes in benefits, employee contributions, the number of eligible employees, or the imposition of any new taxes, fees or assessments by Federal or State regulatory agencies. The Plan reserves the right to make changes to the products available on each tier. All providers are not required to carry all brands on all tiers. For current listing of brands by tier, call 866-939-3633. PLAN DETAILS Quote for group sitused in the State of IN and will be valid until the 09/01/2022 implementation date. Date Quoted 07/18/2022. Rates are valid only when the quoted plan is the sole stand-alone vision plan offered by the group. Percentage discounts are not part of the insurance benefit. Underwritten by Fidelity Security Life Insurance Company of Kansas City, Missouri, except in New York. Fidelity Security Life Policy number VC-146, form number M-9184. PLAN EXCLUSIONS/LIMITATIONS No benefits will be paid for services or materials connected with or charges arising from: medical or surgical treatment, services or supplies for the treatment of the eye, eyes or supporting structures; Refraction, when not provided as part of a Comprehensive Eye Examination; services provided as a result of any Workers’ Compensation law, or similar legislation, or required by any governmental agency or program whether federal, state or subdivisions thereof; orthoptic or vision training, subnormal vision aids and any associated supplemental testing; Aniseikonic lenses; any Vision Examination or any corrective Vision Materials required by a Policyholder as a condition of employment; safety eyewear; solutions, cleaning products or frame cases; non-prescription sunglasses; plano (non-prescription) lenses; plano (non-prescription) contact lenses; two pair of glasses in lieu of bifocals; electronic vision devices; services rendered after the date an Insured Person ceases to be covered under the Policy, except when Vision Materials ordered before coverage ended are delivered, and the services rendered to the Insured Person are within 31 days from the date of such order; or lost or broken lenses, frames, glasses, or contact lenses that are replaced before the next Benefit Frequency when Vision Materials would next become available. Fees charged by a Provider for services other than a covered benefit and any local, state or Federal taxes must be paid in full by the Insured Person to the Provider. Such fees, taxes or materials are not covered under the Policy. Allowances provide no remaining balance for future use within the same Benefit Frequency. Some provisions, benefits, exclusions or limitations listed herein may vary by state. By signing below, the Group agrees to receive all documents and correspondence electronically and that the Group can access the internet or the email address provided. The Group understands that the Group may revoke this authorization or request specific paper documents without revoking this authorization by contacting EyeMed by mail, email, or telephone. If Jay School Corporation has chosen this benefit design, attach this document to the group application and sign here 8/3/2022 | 8:25 AM CDT \d2\ \s2\ Signature Date P201603 TC - 10 Q-00041991 – QL-0000071368
 Fidelity Security Life Insurance Company Group Vision Insurance Policy Page 24
Fidelity Security Life Insurance Company Group Vision Insurance Policy Page 24