
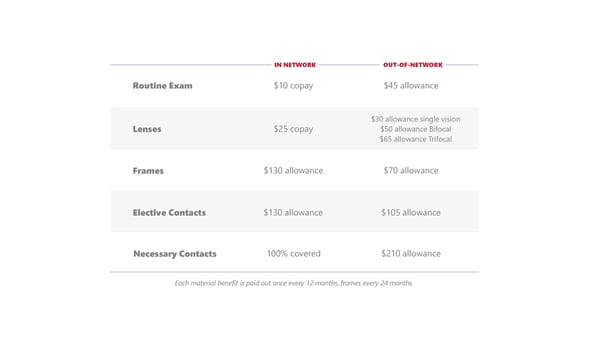
IN NETWORK OUT-OF-NETWORK Routine Exam $10 copay $45 allowance $30 allowance single vision Lenses $25 copay $50 allowance Bifocal $65 allowance Trifocal Frames $130 allowance $70 allowance Elective Contacts $130 allowance $105 allowance Necessary Contacts 100% covered $210 allowance Each material benefit is paid out once every 12 months, frames every 24 months.
 Goshen Community Schools 2025 Benefit Guide Page 19 Page 21
Goshen Community Schools 2025 Benefit Guide Page 19 Page 21