
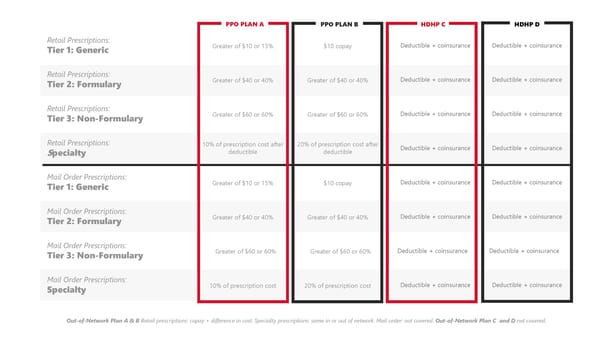
Out-of-Network Plan A & B Retail prescriptions: copay + difference in cost. Specialty prescriptions: same in or out of network. Mail order: not covered. Out-of-Network Plan C and D not covered. Retail Prescriptions: Tier 1: Generic Greater of $10 or 15% $10 copay Deductible + coinsurance Deductible + coinsurance Retail Prescriptions: Tier 2: Formulary Greater of $40 or 40% Greater of $40 or 40% Deductible + coinsurance Deductible + coinsurance Retail Prescriptions: Tier 3: Non-Formulary Greater of $60 or 60% Greater of $60 or 60% Deductible + coinsurance Deductible + coinsurance Retail Prescriptions: Specialty 10% of prescription cost after deductible 20% of prescription cost after deductible Deductible + coinsurance Deductible + coinsurance Mail Order Prescriptions: Tier 1: Generic Greater of $10 or 15% $10 copay Deductible + coinsurance Deductible + coinsurance Mail Order Prescriptions: Tier 2: Formulary Greater of $40 or 40% Greater of $40 or 40% Deductible + coinsurance Deductible + coinsurance Mail Order Prescriptions: Tier 3: Non-Formulary Greater of $60 or 60% Greater of $60 or 60% Deductible + coinsurance Deductible + coinsurance Mail Order Prescriptions: Specialty 10% of prescription cost 20% of prescription cost Deductible + coinsurance Deductible + coinsurance PPO PLAN A PPO PLAN B HDHP C HDHP D
 Goshen Community Schools Employee Benefits Guide Website Page 11 Page 13
Goshen Community Schools Employee Benefits Guide Website Page 11 Page 13