
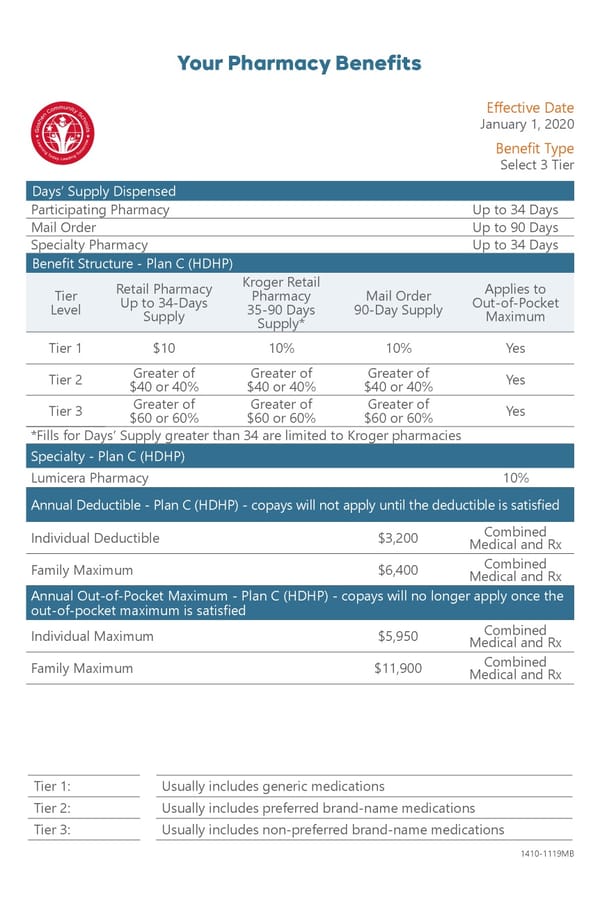
Your Pharmacy Benefits Eff ective Date January 1, 2020 Benefi t Type Select 3 Tier Days’ Supply Dispensed Participating Pharmacy Up to 34 Days Mail Order Up to 90 Days Specialty Pharmacy Up to 34 Days Benefi t Structure - Plan C (HDHP) Kroger Retail Retail Pharmacy Applies to Tier Pharmacy Mail Order Up to 34-Days Out-of-Pocket Level 35-90 Days 90-Day Supply Supply Maximum Supply* Tier 1 $10 10% 10% Yes Greater of Greater of Greater of Tier 2 Yes $40 or 40% $40 or 40% $40 or 40% Greater of Greater of Greater of Tier 3 Yes $60 or 60% $60 or 60% $60 or 60% *Fills for Days’ Supply greater than 34 are limited to Kroger pharmacies Specialty - Plan C (HDHP) Lumicera Pharmacy 10% Annual Deductible - Plan C (HDHP) - copays will not apply until the deductible is satisfi ed Combined Individual Deductible $3,200 Medical and Rx Combined Family Maximum $6,400 Medical and Rx Annual Out-of-Pocket Maximum - Plan C (HDHP) - copays will no longer apply once the out-of-pocket maximum is satisfi ed Combined Individual Maximum $5,950 Medical and Rx Combined Family Maximum $11,900 Medical and Rx Tier 1: Usually includes generic medications Tier 2: Usually includes preferred brand-name medications Tier 3: Usually includes non-preferred brand-name medications 1410-1119MB
 Goshen Community Schools Plan C Page 2 Page 4
Goshen Community Schools Plan C Page 2 Page 4