
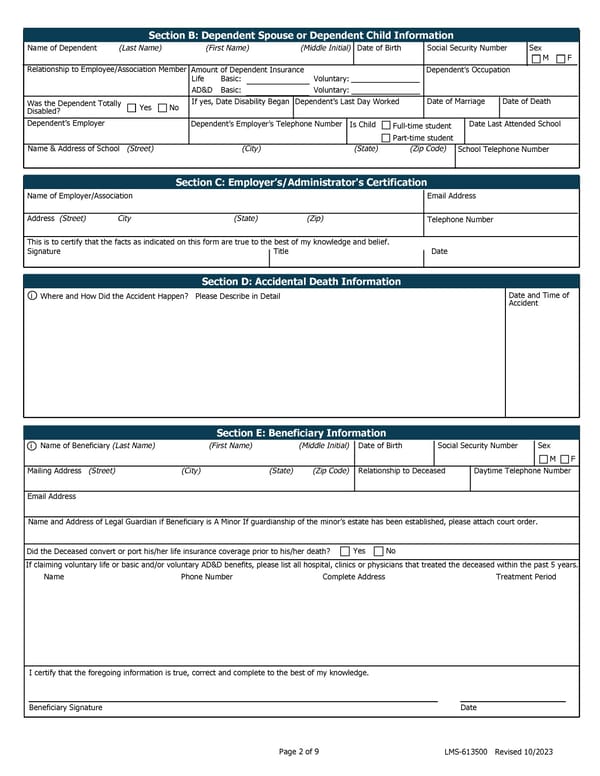
Section B: Dependent Spouse or Dependent Child Information Name of Dependent (Last Name) (First Name) (Middle Initial) Date of Birth Social Security Number Sex M F Relationship to Employee/Association Member Amount of Dependent Insurance Dependent’s Occupation Life Basic: Voluntary: AD&D Basic: Voluntary: Was the Dependent Totally Yes No If yes, Date Disability Began Dependent’s Last Day Worked Date of Marriage Date of Death Disabled? Dependent’s Employer Dependent’s Employer’s Telephone Number Is Child Full-time student Date Last Attended School Part-time student Name & Address of School (Street) (City) (State) (Zip Code) School Telephone Number Section C: Employer’s/Administrator's Certification Name of Employer/Association Email Address Address (Street) City (State) (Zip) Telephone Number This is to certify that the facts as indicated on this form are true to the best of my knowledge and belief. Signature Title Date Section D: Accidental Death Information i Where and How Did the Accident Happen? Please Describe in Detail Date and Time of Accident Section E: Beneficiary Information i Name of Beneficiary (Last Name) (First Name) (Middle Initial) Date of Birth Social Security Number Sex M F Mailing Address (Street) (City) (State) (Zip Code) Relationship to Deceased Daytime Telephone Number Email Address Name and Address of Legal Guardian if Beneficiary is A Minor If guardianship of the minor’s estate has been established, please attach court order. Did the Deceased convert or port his/her life insurance coverage prior to his/her death? Yes No If claiming voluntary life or basic and/or voluntary AD&D benefits, please list all hospital, clinics or physicians that treated the deceased within the past 5 years. Name Phone Number Complete Address Treatment Period I certify that the foregoing information is true, correct and complete to the best of my knowledge. Beneficiary Signature Date Page 2 of 9 LMS-613500 Revised 10/2023
 Group/Association - Proof of Loss: Life Insurance Accidental Death Insurance Page 1 Page 3
Group/Association - Proof of Loss: Life Insurance Accidental Death Insurance Page 1 Page 3