
Group Long Term Disability Claim Form
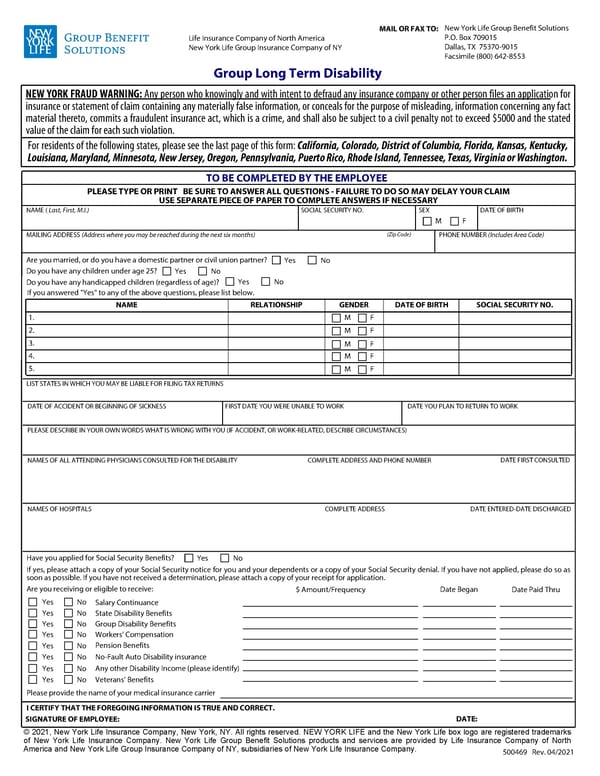
This form is for filing a group long-term disability claim with New York Life Group Benefit Solutions, requiring detailed personal, medical, and employment information from the employee.
500469 Rev. 04/2021 PLEASE DESCRIBE IN YOUR OWN WORDS WHAT IS WRONG WITH YOU (IF ACCIDENT, OR WORK-RELATED, DESCRIBE CIRCUMSTANCES) Are you married, or do you have a domestic partner or civil union partner? Do you have any children under age 25? Do you have any handicapped children (regardless of age)? If you answered "Yes" to any of the above questions, please list below. SOCIAL SECURITY NO. NAME ( Last, First, M.I.) MAILING ADDRESS (Address where you may be reached during the next six months) DATE OF ACCIDENT OR BEGINNING OF SICKNESS FIRST DATE YOU WERE UNABLE TO WORK DATE YOU PLAN TO RETURN TO WORK NAMES OF HOSPITALS COMPLETE ADDRESS NAMES OF ALL ATTENDING PHYSICIANS CONSULTED FOR THE DISABILITY LIST STATES IN WHICH YOU MAY BE LIABLE FOR FILING TAX RETURNS COMPLETE ADDRESS AND PHONE NUMBER DATE FIRST CONSULTED DATE ENTERED-DATE DISCHARGED Please provide the name of your medical insurance carrier 5. If yes, please attach a copy of your Social Security notice for you and your dependents or a copy of your Social Security denial. If you have not applied, please do so as soon as possible. If you have not received a determination, please attach a copy of your receipt for application. 1. Date Paid Thru Salary Continuance State Disability Benefits Group Disability Benefits Workers Compensation Pension Benefits No-Fault Auto Disability insurance Any other Disability Income (please identify) Veterans Benefits Date Began $ Amount/Frequency Are you receiving or eligible to receive: I CERTIFY THAT THE FOREGOING INFORMATION IS TRUE AND CORRECT. SIGNATURE OF EMPLOYEE: DATE: TO BE COMPLETED BY THE EMPLOYEE SEX (Zip Code) PLEASE TYPE OR PRINT BE SURE TO ANSWER ALL QUESTIONS - FAILURE TO DO SO MAY DELAY YOUR CLAIM USE SEPARATE PIECE OF PAPER TO COMPLETE ANSWERS IF NECESSARY DATE OF BIRTH NAME RELATIONSHIP GENDER DATE OF BIRTH SOCIAL SECURITY NO. PHONE NUMBER (Includes Area Code) Have you applied for Social Security Benefits? 2. 3. 4. F M No Yes No Yes No Yes F M F M F M F M F M No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes No Yes NEW YORK FRAUD WARNING: Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance or statement of claim containing any materially false information, or conceals for the purpose of misleading, information concerning any fact material thereto, commits a fraudulent insurance act, which is a crime, and shall also be subject to a civil penalty not to exceed $5000 and the stated value of the claim for each such violation. For residents of the following states, please see the last page of this form: California, Colorado, District of Columbia, Florida, Kansas, Kentucky, Louisiana, Maryland, Minnesota, New Jersey, Oregon, Pennsylvania, Puerto Rico, Rhode Island, Tennessee, Texas, Virginia or Washington. New York Life Group Benefit Solutions P.O. Box 709015 Dallas, TX 75370-9015 Facsimile (800) 642-8553 MAIL OR FAX TO: Life Insurance Company of North America New York Life Group Insurance Company of NY Group Long Term Disability 2021, New York Life Insurance Company, New York, NY. All rights reserved. NEW YORK LIFE and the New York Life box logo are registered trademarks of New York Life Insurance Company. New York Life Group Benefit Solutions products and services are provided by Life Insurance Company of North America and New York Life Group Insurance Company of NY, subsidiaries of New York Life Insurance Company.
 Group Long Term Disability Claim Form Page 2
Group Long Term Disability Claim Form Page 2