
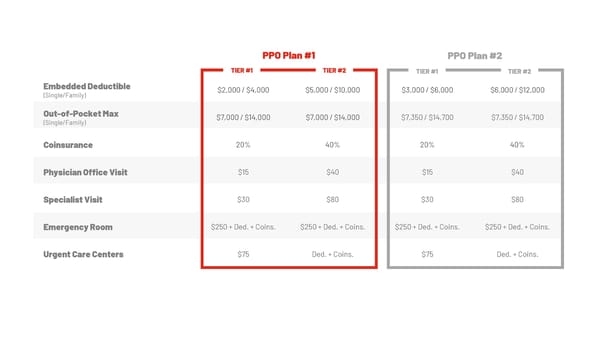
PPO Plan #1 PPO Plan #2 TIER #1 TIER #2 Embedded Deductible (Single/Family) $2,000 / $4,000 $5,000 / $10,000 $3,000 / $6,000 $6,000 / $12,000 Out-of-Pocket Max (Single/Family) $7,000 / $14,000 $7,000 / $14,000 $7,350 / $14,700 $7,350 / $14,700 Coinsurance 20% 40% 20% 40% Physician Office Visit $15 $40 $15 $40 Specialist Visit $30 $80 $30 $80 Emergency Room $250 + Ded. + Coins. $250 + Ded. + Coins. $250 + Ded. + Coins. $250 + Ded. + Coins. Urgent Care Centers $75 Ded. + Coins. $75 Ded. + Coins. TIER #1 TIER #2
 Huntington County Community Schools Benefits Plan 2026 Page 5 Page 7
Huntington County Community Schools Benefits Plan 2026 Page 5 Page 7