
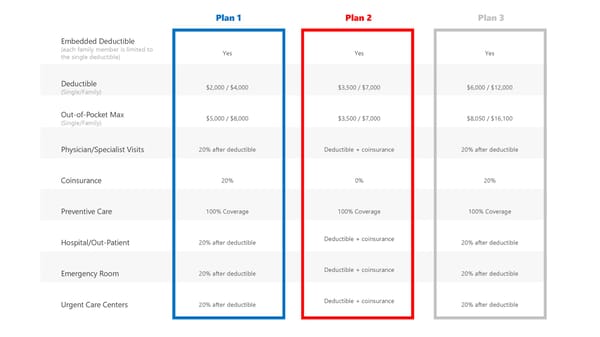
Plan 1 Plan 2 Plan 3 Embedded Deductible (each family member is limited to the single deductible) Yes Yes Yes Deductible (Single/Family) $2,000 / $4,000 $3,500 / $7,000 $6,000 / $12,000 Out-of-Pocket Max (Single/Family) $5,000 / $8,000 $3,500 / $7,000 $8,050 / $16,100 Physician/Specialist Visits 20% after deductible Deductible + coinsurance 20% after deductible Coinsurance 20% 0% 20% Preventive Care 100% Coverage 100% Coverage 100% Coverage Hospital/Out-Patient 20% after deductible Deductible + coinsurance 20% after deductible Emergency Room 20% after deductible Deductible + coinsurance 20% after deductible Urgent Care Centers 20% after deductible Deductible + coinsurance 20% after deductible
 Jay School Corporation Benefits Plan Overview Page 6 Page 8
Jay School Corporation Benefits Plan Overview Page 6 Page 8