
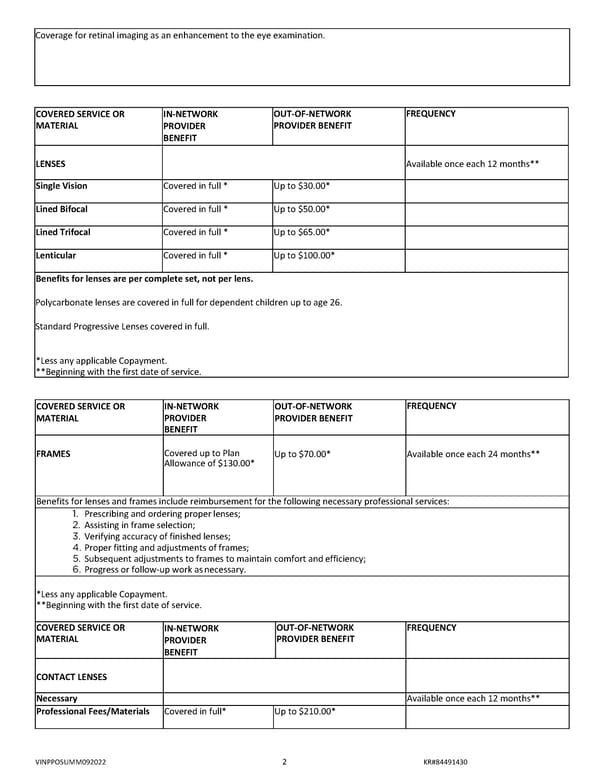
Coverage for retinal imaging as an enhancement to the eye examination. COVERED SERVICE OR IN‐NETWORK OUT‐OF‐NETWORK FREQUENCY MATERIAL PROVIDER PROVIDER BENEFIT BENEFIT LENSES Available once each 12 months** Single Vision Covered in full * Up to $30.00* Lined Bifocal Covered in full * Up to $50.00* Lined Trifocal Covered in full * Up to $65.00* Lenticular Covered in full * Up to $100.00* Benefits for lenses are per complete set, not per lens. Polycarbonate lenses are covered in full for dependent children up to age 26. Standard Progressive Lenses covered in full. *Less any applicable Copayment. **Beginning with the first date of service. COVERED SERVICE OR IN‐NETWORK OUT‐OF‐NETWORK FREQUENCY MATERIAL PROVIDER PROVIDER BENEFIT BENEFIT FRAMES Covered up to Plan Up to $70.00* Available once each 24 months** Allowance of $130.00* Benefits for lenses and frames include reimbursement for the following necessary professional services: 1. Prescribing and ordering proper lenses; 2. Assisting in frame selection; 3. Verifying accuracy of finished lenses; 4. Proper fitting and adjustments of frames; 5. Subsequent adjustments to frames to maintain comfort and efficiency; 6. Progress or follow‐up work as necessary. *Less any applicable Copayment. **Beginning with the first date of service. COVERED SERVICE OR IN‐NETWORK OUT‐OF‐NETWORK FREQUENCY MATERIAL PROVIDER PROVIDER BENEFIT BENEFIT CONTACT LENSES Necessary Available once each 12 months** Professional Fees/Materials Covered in full* Up to $210.00* VINPPOSUMM092022 2 KR#84491430
 Microsoft Word - IN-V0109-0001-2106299-Vision_130_Std_Summary-F0399697 Page 1 Page 3
Microsoft Word - IN-V0109-0001-2106299-Vision_130_Std_Summary-F0399697 Page 1 Page 3