
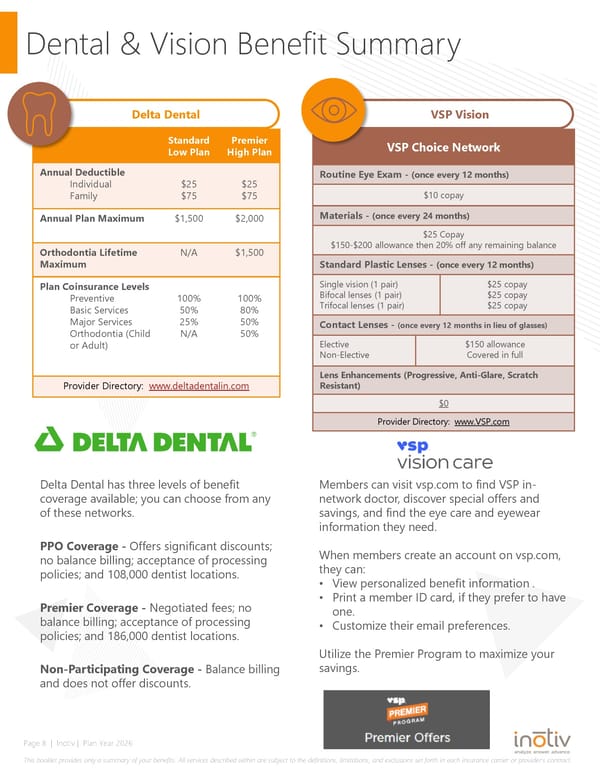
Page 8 | Inotiv | Plan Year 2026 This booklet provides only a summary of your benefits. All services described within are subject to the definitions, limitations, and exclusions set forth in each insurance carrier or providers contract. Dental & Vision Benefit Summary Delta Dental Delta Dental has three levels of benefit coverage available; you can choose from any of these networks. PPO Coverage - Offers significant discounts; no balance billing; acceptance of processing policies; and 108,000 dentist locations. Premier Coverage - Negotiated fees; no balance billing; acceptance of processing policies; and 186,000 dentist locations. Non-Participating Coverage - Balance billing and does not offer discounts. VSP Vision Standard Low Plan Premier High Plan Annual Deductible Individual Family $25 $75 $25 $75 Annual Plan Maximum $1,500 $2,000 Orthodontia Lifetime Maximum N/A $1,500 Plan Coinsurance Levels Preventive Basic Services Major Services Orthodontia (Child or Adult) 100% 50% 25% N/A 100% 80% 50% 50% Provider Directory: www.deltadentalin.com VSP Choice Network Routine Eye Exam - (once every 12 months) $10 copay Materials - (once every 24 months) $25 Copay $150-$200 allowance then 20% off any remaining balance Standard Plastic Lenses - (once every 12 months) Single vision (1 pair) Bifocal lenses (1 pair) Trifocal lenses (1 pair) $25 copay $25 copay $25 copay Contact Lenses - (once every 12 months in lieu of glasses) Elective Non-Elective $150 allowance Covered in full Lens Enhancements (Progressive, Anti-Glare, Scratch Resistant) $0 Provider Directory: www.VSP.com Members can visit vsp.com to find VSP in- network doctor, discover special offers and savings, and find the eye care and eyewear information they need. When members create an account on vsp.com, they can: View personalized benefit information . Print a member ID card, if they prefer to have one. Customize their email preferences. Utilize the Premier Program to maximize your savings.
 New Hire Employee Benefits Guide 2026 Page 7 Page 9
New Hire Employee Benefits Guide 2026 Page 7 Page 9