
Noblesville Schools Bus Driver Benefit Guide
From Plan Year 2025. 1/1/25-12/31/25
Noblesville Schools Bus Driver Benefits 2025 PASSIVE Open Enrollment October 28th – November 8th
Your 2025 Benefits Watch Video Benefits enrollment for 2025 is a passive enrollment period for health, dental, and vision benefits that begin 1/1/2025. If no changes to elections are made, these benefits, in addition to HSA, Voluntary Short-Term Disability, Accident, Critical Illness, Hospital Indemnity, and Voluntary Life Insurance, will roll over to 2025. Flexible spending accounts must be re-enrolled for 2025.
Eligibility Employees Spouse & Legal Dependents Qualifying Events Full-time employees of Noblesville Schools are eligible Your spouse is eligible for medical, dental, and vision as well You may make a change to your benefits if you have a for medical, dental, and vision benefits. as legal dependents up to age 26. Eligible children are qualified status change such as: marriage defined as natural children, legally adopted children, step- divorce, birth/adoption, death, changes in spouse’s Noblesville Schools also provides you with Basic Life children, and children for whom you have legal benefits, and more. and AD&D and Long-Term Disability coverage, at no guardianship. Your children of any age are also eligible if cost to you with the option to purchase Voluntary Life you support them, and they are incapable of self-support and AD&D, Short-Term Disability, Accident, Critical due to disability. Dependents turning 26 are eligible to stay Illness, and Hospital Indemnity Coverages. on the plan until 12/31 of the year they turn 26.
How Does Our Health Plan Work? Carrier Noblesville You Pay Schools Pays Medical Anthem Dental Delta Dental Vision Anthem HSA Contribution Voya Basic Life and AD&D The Standard Voluntary Life The Standard Short-Term Disability The Standard Accident & Hospital Indemnity The Standard
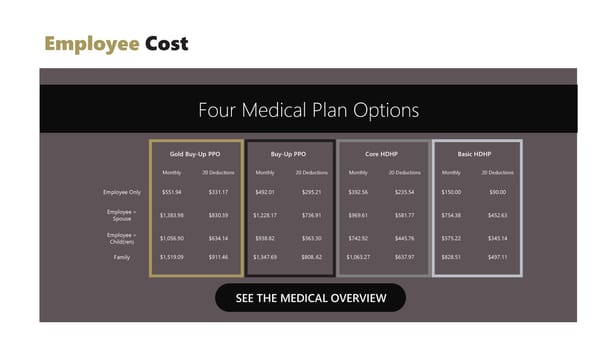
Employee Cost Four Medical Plan Options Gold Buy-Up PPO Buy-Up PPO Core HDHP Basic HDHP Monthly 20 Deductions Monthly 20 Deductions Monthly 20 Deductions Monthly 20 Deductions Employee Only $551.94 $331.17 $492.01 $295.21 $392.56 $235.54 $150.00 $90.00 Employee + $1,383.98 $830.39 $1,228.17 $736.91 $969.61 $581.77 $754.38 $452.63 Spouse Employee + $1,056.90 $634.14 $938.82 $563.30 $742.92 $445.76 $575.22 $345.14 Child(ren) Family $1,519.09 $911.46 $1,347.69 $808..62 $1,063.27 $637.97 $828.51 $497.11 SEE THE MEDICAL OVERVIEW
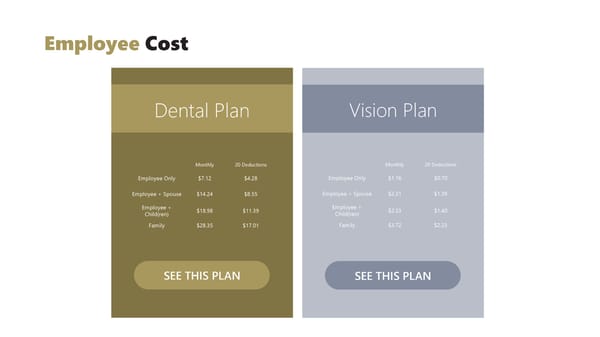
Employee Cost Dental Plan Vision Plan Monthly 20 Deductions Monthly 20 Deductions Employee Only $7.12 $4.28 Employee Only $1.16 $0.70 Employee + Spouse $14.24 $8.55 Employee + Spouse $2.31 $1.39 Employee + $18.98 $11.39 Employee + $2.33 $1.40 Child(ren) Child(ren) Family $28.35 $17.01 Family $3.72 $2.23 SEE THIS PLAN SEE THIS PLAN
Medical BENEFITS All four medicals are administered through Anthem. View Your Anthem Portal
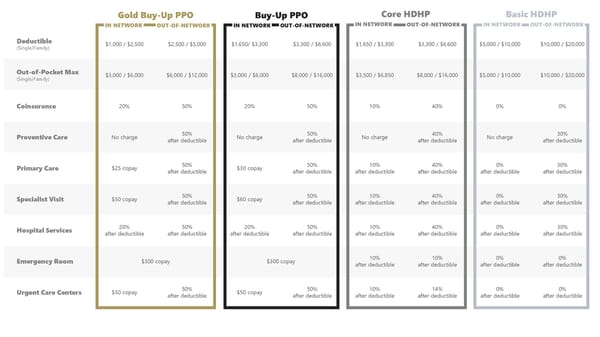
Gold Buy-Up PPO Buy-Up PPO Core HDHP Basic HDHP IN NETWORK OUT-OF-NETWORK IN NETWORK OUT-OF-NETWORK IN NETWORK OUT-OF-NETWORK IN NETWORK OUT-OF-NETWORK Deductible $1,000 / $2,500 $2,500 / $5,000 $1,650/ $3,300 $3,300 / $6,600 $1,650 / $3,300 $3,300 / $6,600 $5,000 / $10,000 $10,000 / $20,000 (Single/Family) Out-of-Pocket Max $3,000 / $6,000 $6,000 / $12,000 $3,000 / $6,000 $8,000 / $16,000 $3,500 / $6,850 $8,000 / $16,000 $5,000 / $10,000 $10,000 / $20,000 (Single/Family) Coinsurance 20% 50% 20% 50% 10% 40% 0% 0% Preventive Care No charge 50% No charge 50% No charge 40% No charge 30% after deductible after deductible after deductible after deductible Primary Care $25 copay 50% $30 copay 50% 10% 40% 0% 30% after deductible after deductible after deductible after deductible after deductible after deductible Specialist Visit $50 copay 50% $60 copay 50% 10% 40% 0% 30% after deductible after deductible after deductible after deductible after deductible after deductible Hospital Services 20% 50% 20% 50% 10% 40% 0% 30% after deductible after deductible after deductible after deductible after deductible after deductible after deductible after deductible Emergency Room $300 copay $300 copay 10% 10% 0% 0% after deductible after deductible after deductible after deductible Urgent Care Centers $50 copay 50% $50 copay 50% 10% 14% 0% 0% after deductible after deductible after deductible after deductible after deductible after deductible
Anthem’s Sydney Health App Manage Your Claims With Sydney Health, you can submit and track your claims, anytime, anywhere. Watch Sydney Health App Video Compare Care & Costs Our digital tools can help you find doctors in your plan’s network and compare care costs up front. Schedule Virtual Appointments Schedule same-day virtual appointments with licensed physicians. Download the App

Prescription DRUGS Your prescription drug plan is through Anthem. Anthem’s CarelonRx is your pharmacy benefit manager. Login to your Anthem portal or Sydney app to view your prescriptions and manage mail-order drugs. Certain specialty medications are administered through Archimedes or Anthem’s Cost Relief program. Eligible members will be contacted directly. Cost Relief Program
Gold Buy-Up PPO Buy-Up PPO Core HDHP Basic HDHP IN NETWORK OUT-OF-NETWORK IN NETWORK OUT-OF-NETWORK IN NETWORK OUT-OF-NETWORK IN NETWORK OUT-OF-NETWORK Retail Prescriptions: 50% 50% 10% 40% 0% 30% Generic $10 copay after deductible, $10 copay after deductible, after deductible after deductible after deductible after deductible Minimum $30 Minimum $30 Retail Prescriptions: 50% 50% 10% 40% 0% 30% Preferred $30 copay after deductible, $30 copay after deductible, after deductible after deductible after deductible after deductible Minimum $30 Minimum $30 Retail Prescriptions: 50% 50% 10% 40% 0% 30% Non-Preferred $75 copay after deductible, $75 copay after deductible, after deductible after deductible after deductible after deductible Minimum $30 Minimum $30 Retail Prescriptions: 50% 50% 10% 40% 0% 0% $300 copay after deductible, $300 copay after deductible, after deductible after deductible after deductible after deductible Specialty Minimum $30 Minimum $30 Mail Order: $10 copay Not covered $10 copay Not covered 10% Not covered 0% Not covered Generic after deductible after deductible Mail Order: $30 copay Not covered $30 copay Not covered 10% Not covered 0% Not covered Preferred after deductible after deductible Mail Order: $75 copay Not covered $75 copay Not covered 10% Not covered 0% Not covered Non-Preferred after deductible after deductible Mail Order: Not covered $300 Copay Not covered 10% Not covered 0% Not covered Specialty $300 Copay after deductible after deductible
Health Savings ACCOUNT A Health Savings Account (HSA) is available to those enrolled in a High Deductible Health Plan. HSA funds can be used for a wide variety of qualified medical expenses all tax-free. Any unused earnings rollover from year-to-year. The 2025 annual max contribution is $4,300 for an individual and $8,550 for families.
Watch This HSA Video to Learn More View Qualified Expenses

HDHP and HSA Consumer Experience Doctor Visit Amount Owed EOB Bill Received Pay with HSA Visit your healthcare provider and The health plan will share the The health plan send you the Your doctor will then send you You can use your HSA funds the office will submit the claim to amount you owe with your Explanation of Benefits (EOB). a bill. to pay the bill from your your health plan. doctor. doctor.
DENTAL DELTA DENTAL OF INDIANA 225 S East St Indianapolis, IN 46202 317-842-4022 Dental Coverage with Delta Dental KRISTEN JONES Group Delta Dental PPO For the highest benefit levels, we encourage you to select a provider from Delta Dental’s extensive network. You may pay less out of your pocket. Online Portal Download the App
IN NETWORK OUT-OF-NETWORK Deductible No deductible $25 Annual Plan Maximum $1,250 (Maximum Per Person) Preventive Services You Pay 0% Exams, Cleanings, Fluoride, X-Rays Basic Services You Pay 10% You Pay 15% Fillings, Extractions, Endodontics, Crown Repairs Major Services You Pay 40% You Pay 45% Crowns, Dentures, In/Outlays, Periodontics Orthodontia Services You Pay 50% (maximum age limit 18) Orthodontia Lifetime Maximum $1,250 $1,000
VISION Vision Coverage with Anthem For the highest benefit levels, we encourage you to select a provider from Anthem’s extensive network. You may pay less out of your pocket. View Your Anthem Portal
IN NETWORK OUT-OF-NETWORK Exam $10 copay Up to $42 Glasses Lenses Up to $40 (Single / Bifocal/ Trifocal / Lenticular) $15 copay Up to $60 Up to $85 Glasses Frames $15 copay, then $130 allowance, Up to $45 20% off remaining balance Contact Lenses $15 copay, then $130 allowance, Up to $210/$105 (Medically Necessary & Elective) 20% off remaining balance Each material benefit is paid out once per calendar year.
4 Ways to SAVE ON HEALTHCARE AVOID CUT Rx SHOP STAY THE ER COST AROUND HEALTHY FOR TRUE EMERGENCIES DON’T COMPARE DRUG PRICES & TALK UTILIZE THE SYDNEY APP TO FIND LIVE A HEALTHY LIFESTYLE HESITATE TO CALL 911 OR GO TO TO YOUR DOCTOR ABOUT THE BEST CARE AT THE BEST PRICE. THROUGH REGULAR MOVEMENT THE EMERGENCY ROOM. LOWER COST OPTIONS. & HEALTHY EATING HABITS. CHECK DISCOUNTS IN THE SYDNEY WHEN POSSIBLE, UTILIZING A UTILIZE COUPONS & SERVICES APP FOR MEDICAL TREATMENTS, REGULARLY VISIT YOUR WALK-IN CLINIC OR URGENT LIKE GOODRx, Rx HELP CENTERS, DENTAL, VISION, HEARING, PRIMIARY CARE PHYSICIAN. CARE WILL SAVE YOU TIME AND OR THE COSTPLUS DRUG FITNESS, FAMILY, PETS, & MORE. MONEY FOR THE SAME COMPANY. SERVICES. SCHEDULE YOUR ANNUAL LAB WORK & IMAGING SERVICES PHYSICAL & PREVENTIVE CARE LIKE ULTRASOUNDS, X-RAYS, CT APPOINTMENTS. SCANS, BLOOD DRAWS, ETC. ARE COSTLY. RESEARCH PROVIDERS BEFORE YOU MAKE AN APPT. $ $$ $$$ $$$$
Additional BENEFITS Noblesville Schools provides additional benefit opportunities.
Flexible Spending Accounts Watch This FSA Video to Learn 1 Flexible Spending Accounts (FSA) are set up to pay for many of out-of- More pocket medical expenses with tax-free dollars. The FSA account holder GENERAL sets aside a pre-tax dollar amount for the year used to pay for medical PURPOSE FSA expenses. Unused FSA funds can expire at the end of the year. General Purpose FSA 1 An FSA is an alternative to an HSA. FSAs are typically paired with a PPO plan while an HSA is paired with an HDHP. HSA funds can 2 be used on various medical, dental, and vision related expenses. View Eligible Expenses DEPENDENT CARE ACCOUNT Dependent Care Account (DCA) 2 A DCA is a tax-free spending account for dependent care expenses such as daycare, preschool, or day camps for any dependent under the age of 13 or who is physically or mentally incapable of self-care. Learn More About Your DCA
Basic Life Insurance Voluntary Life & AD&D The Noblesville Schools employer-paid basic life insurance Employee Benefit: Increments of $1,000 up to $500,000. policy is available to all full-time employees. In the event of Guarantee issue of $300,000. your death, your beneficiaries will receive $30,000. Coverage Spouse Benefit: Increments of $5,000 up to $250,000. decreases incrementally at age 65. (Cannot exceed 50% of employee amount) Guarantee issue of $25,000. Child(ren) Benefit: Up to $2,500 up to $10,000. Guarantee issue is $10,000. Basic Accidental Death & (Children age 14 days to 23 years, 26 if full-time student) Dismemberment Insurance Short-Term Disability The Noblesville Schools employer-paid basic AD&D Employee-paid short-term disability protects your income insurance policy is available to all full-time employees. In during a short period of time due to illness, maternity leave, the event of death, loss of (or loss of use of) a body part or an accident not related to your job. or function, speech, eyesight, or hearing, your beneficiaries will receive $30,000. Coverage decreases Benefits begin on the 7th day after the date of the incident incrementally at age 65. and will cover 662/3% of your weekly earnings up to $1,750. Click To Calculate Your Premium
Accident Up to $3,400 cash benefits that correspond with hospital and intensive care confinement. Your plan may also include coverage for a variety of occurrences, such as dismemberment; dislocation or fracture; ambulance services; physical therapy and more. Learn More Critical Illness Employee & Spouse Benefit: $5,000 to $30,000 (Spouse cannot exceed employee coverage amount). Child(ren) Benefit: 50% of employee benefit. View Monthly Premiums Hospital Indemnity The Standard coverage pays you cash benefits that correspond with hospital admission, confinement and intensive care confinement. View Benefit Amounts & Premiums
Pay and Deduction Calendar Pay Date 24 Deduction 20 Deduction Beginning Ending Pay Day JANUARY FEBRUARY MARCH APRIL 12/8/24 12/21/24 1/3/25 12/22/24 1/4/25 1/17/25 1 2 3 4 1 1 1 2 3 4 5 1/5/25 1/18/25 1/31/25 5 6 7 8 9 10 11 2 3 4 5 6 7 8 2 3 4 5 6 7 8 6 7 8 9 10 11 12 1/19/25 2/1/25 2/14/25 12 13 14 15 16 17 18 9 10 11 12 13 14 15 9 10 11 12 13 14 15 13 14 15 16 17 18 19 2/2/25 3/1/25 2/28/25 2/16/25 3/15/25 3/14/25 19 20 21 22 23 24 25 16 17 18 19 20 21 22 16 17 18 19 20 21 22 20 21 22 23 24 25 26 3/2/25 3/29/25 3/18/25 26 27 28 29 30 31 23 24 25 26 27 28 23/ 24/ 25 29 27 28 29 27 28 29 30 3/16/25 4/12/25 4/11/25 30 31 MAY JUNE JULY AUGUST 3/30/25 4/26/25 4/25/25 4/13/25 5/10/25 5/9/25 1 2 3 1 2 3 4 5 6 7 1 2 3 4 5 1 2 4/27/25 5/24/25 5/23/25 4 5 6 7 8 9 10 8 9 10 11 12 13 14 6 7 8 9 10 11 12 3 4 5 6 7 8 9 5/11/25 6/7/25 6/6/25 11 12 13 14 15 16 17 15 16 17 18 19 20 21 13 14 15 16 17 18 19 10 11 12 13 14 15 16 5/25/25 6/21/25 6/20/25 6/8/25 7/5/25 7/4/25 18 19 20 21 22 23 24 22 23 24 25 26 27 28 20 21 22 23 24 25 26 17 18 19 20 21 22 23 6/22/25 7/19/25 7/18/25 25 26 27 28 29 30 31 29 30 27 28 29 30 31 24/ 25 26 27 28 29 30 7/6/25 8/2/25 8/1/25 31 7/20/25 8/16/25 8/15/25 SEPTEMBER OCTOBER NOVEMBER DECEMBER 8/3/25 8/16/25 8/29/25 1 2 3 4 5 6 1 2 3 4 1 1 2 3 4 5 6 8/17/25 8/30/25 9/12/25 7 8 9 10 11 12 13 5 6 7 8 9 10 11 2 3 4 5 6 7 8 7 8 9 10 11 12 13 8/31/25 9/13/25 9/26/25 14 15 16 17 18 19 20 12 13 14 15 16 17 18 9 10 11 12 13 14 15 14 15 16 17 18 19 20 9/14/25 9/27/25 10/10/25 9/28/25 10/11/25 10/24/25 21 22 23 24 25 26 27 19 20 21 22 23 24 25 16 17 18 19 20 21 22 21 22 23 24 25 26 27 10/12/25 10/24/25 11/7/25 28 29 30 26 27 28 29 30 31 23/ 24 25 26 27 28 29 28 29 30 31 10/26/25 11/8/25 11/21/25 30 11/9/25 11/22/25 12/5/25 11/23/25 12/6/25 12/19/25
PlanSource Get Enrolled Today! st User: Fname Initial + 1 6 letters of Lname + last 4 digits of SSN Password: Birthday in format of YYYY/MM/DD Enroll Online