Noblesville Schools COBRA Benefits 2026
This document outlines the COBRA benefits available for the 2026 plan year at Noblesville Schools.
2026 Plan Year Noblesville Schools COBRA Benefits
Employee Monthly Cost Employee Only $926.61 $802.87 $712.95 $36.30 $5.88 Employee + Spouse $2,283.07 $1,964.08 $1,762.76 $72.58 $11.75 Employee + Child(ren) $1,748.95 $1,506.85 $1,349.40 $96.80 $11.87 Family $2,503.49 $2,152.77 $1,933.45 $144.54 $18.94 Surest Core HDHP Basic HDHP Dental Vision
Medical BENEFITS All three medical plans are administered through UHC/Surest. View Your UHC Portal View Your Surest Portal
Upfront Pricing No deductibles. No coinsurance. Copay-only plan with lower out-of-pocket costs. Find Care Quickly Find the care you need on the Surest app or website. Compare & Save Check costs and compare options before you make an appointment. Learn More About Surest Watch the Surest “How it Works” Video UnitedHealthcare’s Surest Health Plan Download App
View Your Claims Check the status of new and past claims. See the amount billed, what your plan paid and how much you owe. Find Care & Pricing Search for network providers near you, see ratings and reviews, and estimate out-of-pocket costs. Access Your ID Card Your digital ID card is always with you when you need it. UnitedHealthcare Mobile App Download the App
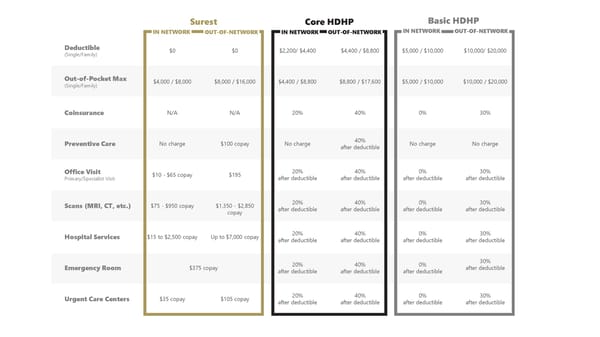
Deductible (Single/Family) $0 $0 $2,200/ $4,400 $4,400 / $8,800 $5,000 / $10,000 $10,000/ $20,000 Out-of-Pocket Max (Single/Family) $4,000 / $8,000 $8,000 / $16,000 $4,400 / $8,800 $8,800 / $17,600 $5,000 / $10,000 $10,000 / $20,000 Coinsurance N/A N/A 20% 40% 0% 30% Preventive Care No charge $100 copay No charge 40% after deductible No charge No charge Office Visit Primary/Specialist Visit $10 - $65 copay $195 20% after deductible 40% after deductible 0% after deductible 30% after deductible Scans (MRI, CT, etc.) $75 - $950 copay $1,350 - $2,850 copay 20% after deductible 40% after deductible 0% after deductible 30% after deductible Hospital Services $15 to $2,500 copay Up to $7,000 copay 20% after deductible 40% after deductible 0% after deductible 30% after deductible Emergency Room $375 copay 20% after deductible 40% after deductible 0% after deductible 30% after deductible Urgent Care Centers $35 copay $105 copay 20% after deductible 40% after deductible 0% after deductible 30% after deductible Surest Core HDHP IN NETWORK OUT-OF-NETWORK IN NETWORK OUT-OF-NETWORK Basic HDHP IN NETWORK OUT-OF-NETWORK
Prescription DRUGS Your prescription drug plan is through CVS Caremark. CVS Caremark is your pharmacy benefit manager. The Caremark network includes most retail chain pharmacies such as Walgreens, CVS, Walmart, Meijer, Kroger, and Costco. Mail order prescriptions can be ordered directly through Caremark. A preventive drug list can be found using the Caremark Portal link below. Caremark Portal
Retail Prescriptions: Generic $10 copay 50% after deductible, Minimum $30 20% after deductible 40% after deductible 0% after deductible 30% after deductible Retail Prescriptions: Preferred $30 copay 50% after deductible, Minimum $30 20% after deductible 40% after deductible 0% after deductible 30% after deductible Retail Prescriptions: Non-Preferred $75 copay 50% after deductible, Minimum $30 20% after deductible 40% after deductible 0% after deductible 30% after deductible Retail Prescriptions: Specialty $300 copay 50% after deductible, Minimum $30 20% after deductible 40% after deductible 0% after deductible 0% after deductible Mail Order: Generic $10 copay Not covered 20% after deductible Not covered 0% after deductible Not covered Mail Order: Preferred $65 copay Not covered 20% after deductible Not covered 0% after deductible Not covered Mail Order: Non-Preferred $145 copay Not covered 20% after deductible Not covered 0% after deductible Not covered Mail Order: Specialty $300 Copay Not covered 20% after deductible Not covered 0% after deductible Not covered Surest Core HDHP IN NETWORK OUT-OF-NETWORK IN NETWORK OUT-OF-NETWORK Basic HDHP IN NETWORK OUT-OF-NETWORK

DENTAL For the highest benefit levels, we encourage you to select a provider from Delta Dental’s extensive network. You may pay less out of your pocket. Dental Coverage with Delta Dental DELTA DENTAL OF INDIANA 225 S East St Indianapolis, IN 46202 317-842-4022 KRISTEN JONES Group Delta Dental PPO Online Portal Download the App
Deductible No deductible $25 Annual Plan Maximum $1,250 (Maximum Per Person) Preventive Services Exams, Cleanings, Fluoride, X-Rays You Pay 0% Basic Services Fillings, Extractions, Endodontics, Crown Repairs You Pay 10% You Pay 15% Major Services Crowns, Dentures, In/Outlays, Periodontics You Pay 40% You Pay 45% Orthodontia Services (maximum age limit 18) You Pay 50% Orthodontia Lifetime Maximum $1,250 $1,000 IN NETWORK OUT-OF-NETWORK
VISION For the highest benefit levels, we encourage you to select a provider from Anthem’s extensive network. You may pay less out of your pocket. Vision Coverage with Anthem View Your Anthem Portal
Each material benefit is paid out once per calendar year. Exam $10 copay Up to $42 Glasses Lenses (Single / Bifocal/ Trifocal / Lenticular) $15 copay Up to $40 Up to $60 Up to $85 Glasses Frames $15 copay, then $130 allowance, 20% off remaining balance Up to $45 Contact Lenses (Medically Necessary & Elective) $15 copay, then $130 allowance, 20% off remaining balance Up to $210/$105 IN NETWORK OUT-OF-NETWORK
PlanSource User: Fname Initial + 1st 6 letters of Lname + last 4 digits of SSN Password: Birthday in format of YYYY/MM/DD Get Enrolled Today! Enroll Online