
Noblesville Schools COBRA Benefits
Noblesville Schools COBRA Benefits 2025 Plan Year
Employee Monthly Cost Gold Buy-Up Buy-Up PPO Core HDHP Basic HDHP Dental Vision PPO Employee Only $948.04 $886.91 $785.47 $697.79 $36.30 $5.88 Employee + $2,344.18 $2,185.25 $1,921.52 $1,725.28 $72.58 $11.75 Spouse Employee + $1,794.45 $1,674.02 $1,474.19 $1,320.71 $96.80 $11.87 Child(ren) Family $2,571.05 $2,396.23 $2,106.11 $1,892.34 $144.54 $18.94
Medical BENEFITS All four medicals are administered through Anthem. View Your Anthem Portal
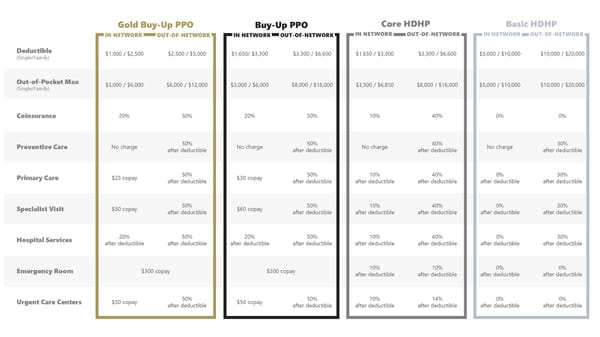
Gold Buy-Up PPO Buy-Up PPO Core HDHP Basic HDHP IN NETWORK OUT-OF-NETWORK IN NETWORK OUT-OF-NETWORK IN NETWORK OUT-OF-NETWORK IN NETWORK OUT-OF-NETWORK Deductible $1,000 / $2,500 $2,500 / $5,000 $1,650/ $3,300 $3,300 / $6,600 $1,650 / $3,300 $3,300 / $6,600 $5,000 / $10,000 $10,000 / $20,000 (Single/Family) Out-of-Pocket Max $3,000 / $6,000 $6,000 / $12,000 $3,000 / $6,000 $8,000 / $16,000 $3,500 / $6,850 $8,000 / $16,000 $5,000 / $10,000 $10,000 / $20,000 (Single/Family) Coinsurance 20% 50% 20% 50% 10% 40% 0% 0% Preventive Care No charge 50% No charge 50% No charge 40% No charge 30% after deductible after deductible after deductible after deductible Primary Care $25 copay 50% $30 copay 50% 10% 40% 0% 30% after deductible after deductible after deductible after deductible after deductible after deductible Specialist Visit $50 copay 50% $60 copay 50% 10% 40% 0% 30% after deductible after deductible after deductible after deductible after deductible after deductible Hospital Services 20% 50% 20% 50% 10% 40% 0% 30% after deductible after deductible after deductible after deductible after deductible after deductible after deductible after deductible Emergency Room $300 copay $300 copay 10% 10% 0% 0% after deductible after deductible after deductible after deductible Urgent Care Centers $50 copay 50% $50 copay 50% 10% 14% 0% 0% after deductible after deductible after deductible after deductible after deductible after deductible
Prescription DRUGS Your prescription drug plan is through Anthem.
Gold Buy-Up PPO Buy-Up PPO Core HDHP Basic HDHP IN NETWORK OUT-OF-NETWORK IN NETWORK OUT-OF-NETWORK IN NETWORK OUT-OF-NETWORK IN NETWORK OUT-OF-NETWORK Retail Prescriptions: 50% 50% 10% 40% 0% 30% Generic $10 copay after deductible, $10 copay after deductible, after deductible after deductible after deductible after deductible Minimum $30 Minimum $30 Retail Prescriptions: 50% 50% 10% 40% 0% 30% Preferred $30 copay after deductible, $30 copay after deductible, after deductible after deductible after deductible after deductible Minimum $30 Minimum $30 Retail Prescriptions: 50% 50% 10% 40% 0% 30% Non-Preferred $75 copay after deductible, $75 copay after deductible, after deductible after deductible after deductible after deductible Minimum $30 Minimum $30 Retail Prescriptions: 50% 50% 10% 40% 0% 0% $300 copay after deductible, $300 copay after deductible, after deductible after deductible after deductible after deductible Specialty Minimum $30 Minimum $30 Mail Order: $10 copay Not covered $10 copay Not covered 10% Not covered 0% Not covered Generic after deductible after deductible Mail Order: $30 copay Not covered $30 copay Not covered 10% Not covered 0% Not covered Preferred after deductible after deductible Mail Order: $75 copay Not covered $75 copay Not covered 10% Not covered 0% Not covered Non-Preferred after deductible after deductible Mail Order: Not covered $300 Copay Not covered 10% Not covered 0% Not covered Specialty $300 Copay after deductible after deductible
DENTAL DELTA DENTAL OF INDIANA 225 S East St Indianapolis, IN 46202 317-842-4022 Dental Coverage with Delta Dental KRISTEN JONES Group Delta Dental PPO For the highest benefit levels, we encourage you to select a provider from Delta Dental’s extensive network. You may pay less out of your pocket. Online Portal Download the App
IN NETWORK OUT-OF-NETWORK Deductible No deductible $25 Annual Plan Maximum $1,250 (Maximum Per Person) Preventive Services You Pay 0% Exams, Cleanings, Fluoride, X-Rays Basic Services You Pay 10% You Pay 15% Fillings, Extractions, Endodontics, Crown Repairs Major Services You Pay 40% You Pay 45% Crowns, Dentures, In/Outlays, Periodontics Orthodontia Services You Pay 50% (maximum age limit 18) Orthodontia Lifetime Maximum $1,250 $1,000
VISION Vision Coverage with Anthem For the highest benefit levels, we encourage you to select a provider from Anthem’s extensive network. You may pay less out of your pocket. View Your Anthem Portal
IN NETWORK OUT-OF-NETWORK Exam $10 copay Up to $42 Up to $40 Glasses Lenses $15 copay Up to $60 (Single / Bifocal/ Trifocal / Lenticular) Up to $85 Glasses Frames $15 copay, then $130 allowance, Up to $45 20% off remaining balance Contact Lenses $15 copay, then $130 allowance, Up to $210/$105 (Medically Necessary & Elective) 20% off remaining balance Each material benefit is paid out once per calendar year.
PlanSource Get Enrolled Today! st User: Fname Initial + 1 6 letters of Lname + last 4 digits of SSN Password: Birthday in format of YYYY/MM/DD Enroll Online