
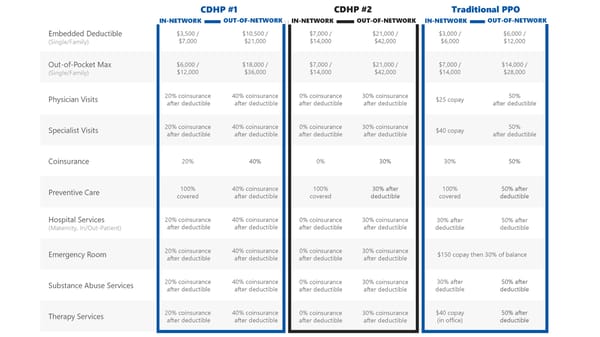
Embedded Deductible (Single/Family) $3,500 / $7,000 $10,500 / $21,000 $7,000 / $14,000 $21,000 / $42,000 $3,000 / $6,000 $6,000 / $12,000 Out-of-Pocket Max (Single/Family) $6,000 / $12,000 $18,000 / $36,000 $7,000 / $14,000 $21,000 / $42,000 $7,000 / $14,000 $14,000 / $28,000 Physician Visits 20% coinsurance after deductible 40% coinsurance after deductible 0% coinsurance after deductible 30% coinsurance after deductible $25 copay 50% after deductible Specialist Visits 20% coinsurance after deductible 40% coinsurance after deductible 0% coinsurance after deductible 30% coinsurance after deductible $40 copay 50% after deductible Coinsurance 20% 40% 0% 30% 30% 50% Preventive Care 100% covered 40% coinsurance after deductible 100% covered 30% after deductible 100% covered 50% after deductible Hospital Services (Maternity, In/Out-Patient) 20% coinsurance after deductible 40% coinsurance after deductible 0% coinsurance after deductible 30% coinsurance after deductible 30% after deductible 50% after deductible Emergency Room 20% coinsurance after deductible 40% coinsurance after deductible 0% coinsurance after deductible 30% coinsurance after deductible $150 copay then 30% of balance Substance Abuse Services 20% coinsurance after deductible 40% coinsurance after deductible 0% coinsurance after deductible 30% coinsurance after deductible 30% after deductible 50% after deductible Therapy Services 20% coinsurance after deductible 40% coinsurance after deductible 0% coinsurance after deductible 30% coinsurance after deductible $40 copay (in office) 50% after deductible CDHP #1 CDHP #2 Traditional PPO OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK IN-NETWORK OUT-OF-NETWORK IN-NETWORK
 Online Transport 2025 Benefit Guide Page 6 Page 8
Online Transport 2025 Benefit Guide Page 6 Page 8